Chronic cortisol does not just stay high. It changes what your cells do with it.
Cortisol is not the villain most wellness content makes it. It is a hormone that keeps you alive, wakes you up, and lets you respond to threat. The problem is not cortisol itself. It is what happens when the acute stress response never gets to switch off. Chronic elevation triggers a second failure most articles skip entirely: glucocorticoid receptor resistance. Your cells stop listening to cortisol correctly, which explains why chronic stress causes inflammation, weight redistribution, memory loss, immune dysfunction, hormonal collapse, and sleep disruption at the same time. This is the complete research overview of what chronic cortisol actually does, with links to every mechanism in depth.
Almost everything you have read about cortisol is either too simple or wrong. Too simple: cortisol is bad, lower it. Wrong: adrenal fatigue is causing your symptoms. What the research actually shows is more nuanced, more interesting, and more useful.
Chronic stress does not just keep cortisol high. It reshapes how your body uses cortisol at the cellular level. The hormone can be elevated while your cells simultaneously act as if there is not enough of it. That contradiction, which is called glucocorticoid receptor resistance, explains why chronic stress causes so many symptoms at once and why so many wellness interventions fail to move the needle.
This guide covers the complete picture. What cortisol actually does. How the daily rhythm works. What happens during acute stress. Where and how the system breaks under chronic load. And what each downstream system, from belly fat to memory to sleep, is doing when cortisol dysregulation takes over. Each section connects to a deeper research piece if you want to go further.
Cortisol is not the villain. The pattern is.
Cortisol is a steroid hormone produced by the adrenal glands, two small structures sitting on top of your kidneys. It belongs to a class called glucocorticoids. The name comes from its role in raising blood glucose during moments of demand, but that description undersells everything else it does.
Beyond glucose regulation, cortisol wakes you up in the morning. It stabilizes blood pressure when you stand up, gives you daytime energy, and coordinates the shift between fed and fasted states. Immune activity relies on it to curb inflammation when you are healthy. Memory consolidation during sleep needs it. Without cortisol, you would not survive twenty-four hours.
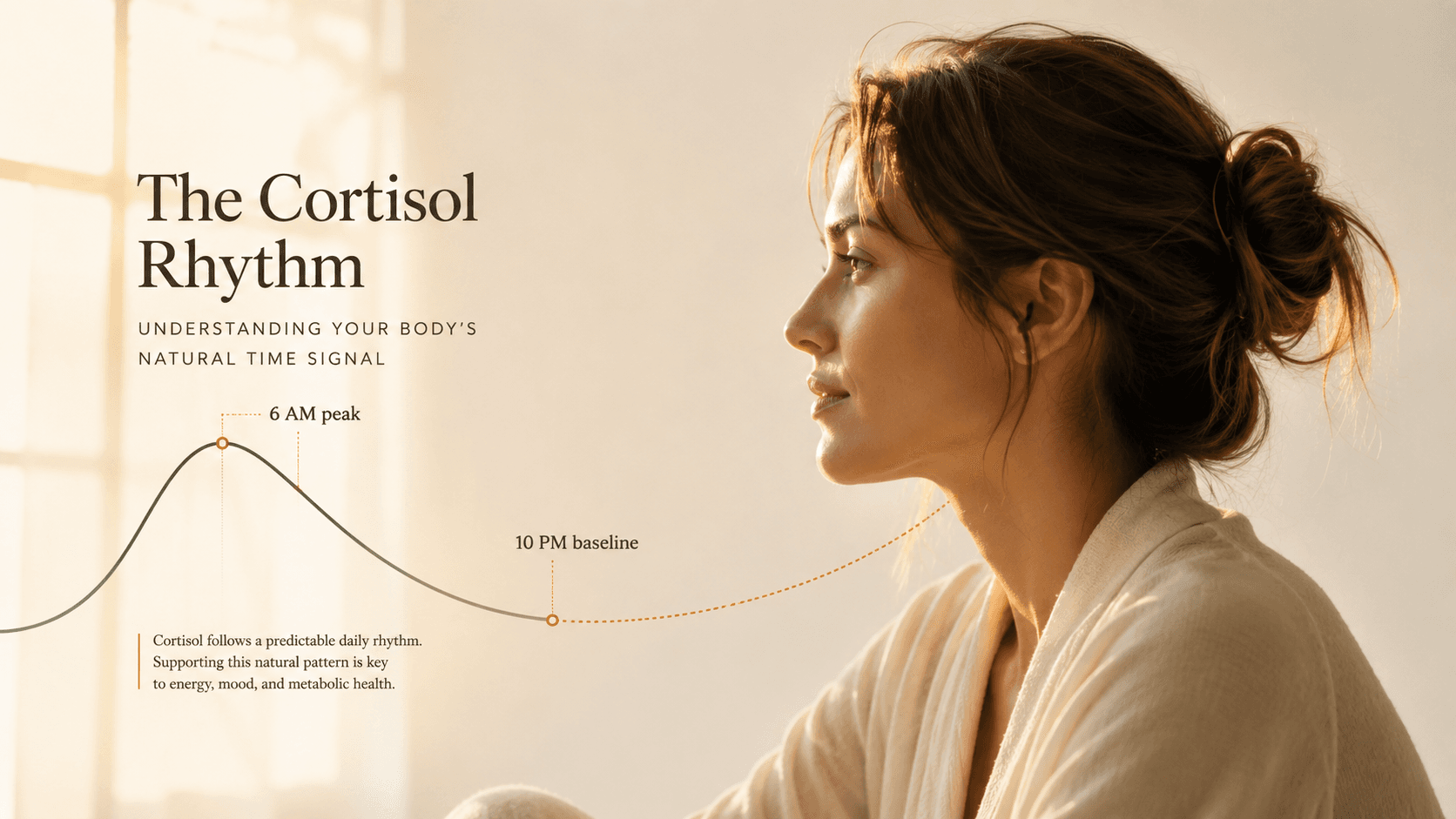
The reason most cortisol articles feel useless is that they treat cortisol as a single number. It is not. Cortisol is a wave. A high morning peak. A steady daytime slope. A near-zero nighttime baseline. Health is defined by the shape of the wave, not the height of any single point. When the rhythm flattens, disease follows. When the rhythm is sharp and predictable, the same absolute levels are protective.
The framing matters because it changes what you are trying to fix. You are not trying to lower cortisol. You are trying to restore the rhythm. Those two goals sometimes align and sometimes diverge, and the difference explains a lot about why cortisol advice online tends to contradict itself.
→The foundational readWhat Cortisol Actually Does: The Stress Hormone Explained Beyond the Wellness PanicHow healthy cortisol actually flows through the day
The normal cortisol curve begins about three hours before you wake up. Levels rise slowly during the last cycles of sleep, then surge sharply thirty to forty-five minutes after opening your eyes. This surge has a specific name: the cortisol awakening response, or CAR.
The CAR is not a bug. It is the reason you can get out of bed. It mobilizes glucose, sharpens attention, and primes the cardiovascular system for the demands of the day. In healthy adults, the CAR raises cortisol by 50 to 75 percent above baseline within an hour of waking.
After the peak, cortisol declines throughout the day in a fairly linear slope. By evening, levels are a fraction of morning values. Around midnight, cortisol reaches its lowest point, which is when growth hormone rises, deep sleep dominates, and tissue repair happens.
A healthy day of cortisol
- 3-6 AMExpected
Cortisol begins to rise, preparing you to wake.
- 6-9 AMExpected
The CAR peaks 30-45 minutes after waking. Alertness surges.
- 9 AM to 6 PMExpected
Steady decline. Energy sustained through work and activity.
- 6-10 PMExpected
Cortisol drops toward baseline. Body prepares for repair.
- 10 PM to 3 AMVisible result
Cortisol at its lowest. Growth hormone peaks. Deep sleep dominates.
When this rhythm holds, you feel awake in the morning, energetic through the afternoon, calm in the evening, and asleep through the night. When it breaks, every one of those states inverts. Morning brain fog, afternoon crashes, evening anxiety, 3 AM waking. Same hormone. Different pattern.
→Morning anxiety decodedWhy You Wake Up Anxious: The Cortisol Awakening Response Nobody ExplainsWhat cortisol does during an actual threat
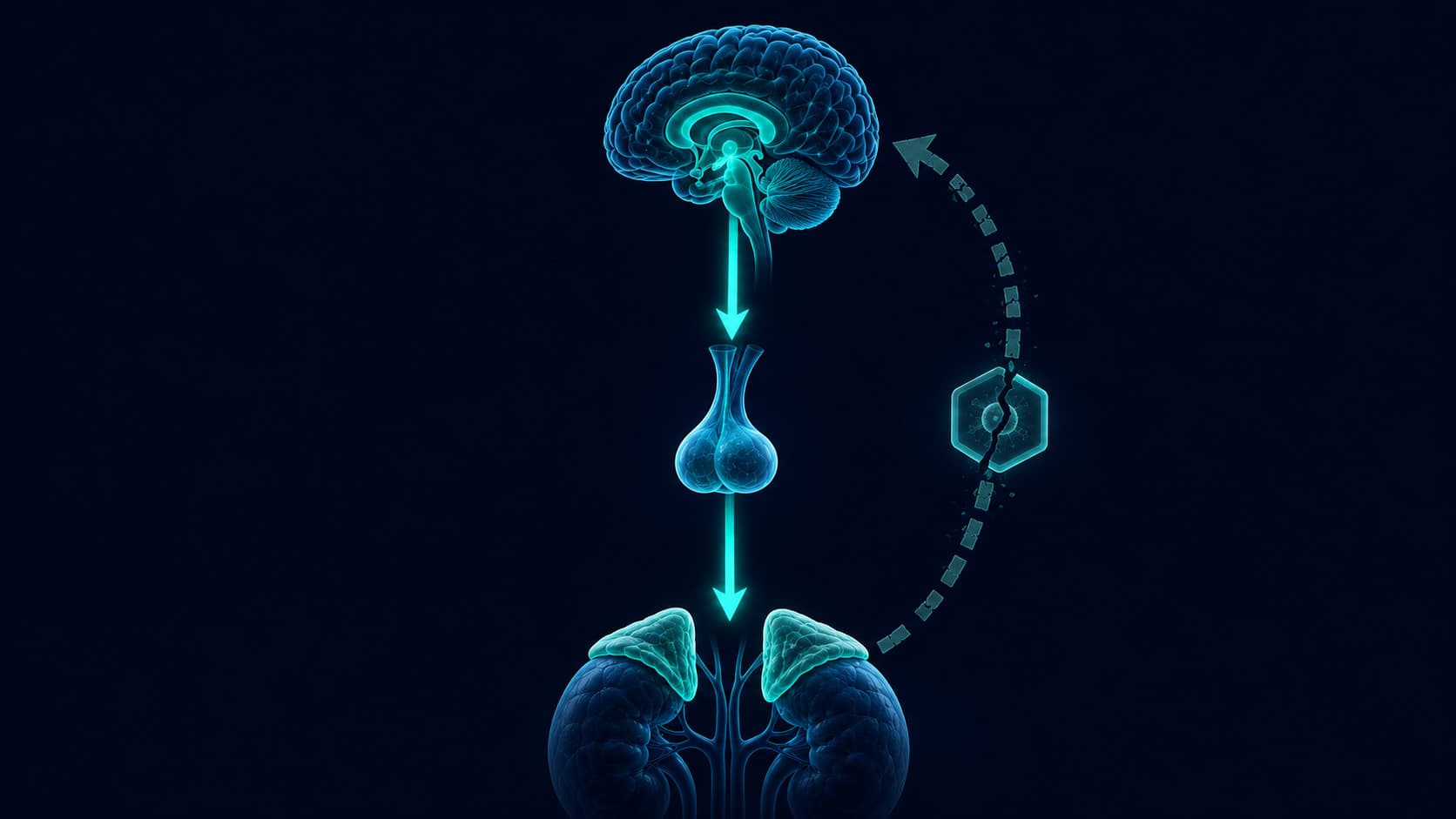
Acute stress activates a specific cascade. The hypothalamus in your brain detects the threat and releases corticotropin-releasing hormone. That signal travels a short distance to the pituitary gland, which releases adrenocorticotropic hormone into the bloodstream. ACTH reaches the adrenal cortex and triggers cortisol release within minutes.
This entire sequence, called the HPA axis, exists so that when your ancestors saw a predator, they could sprint, fight, or freeze appropriately. In modern life, the HPA axis fires for deadlines, arguments, financial stress, traffic, and doomscrolling. The hardware does not distinguish between a saber-toothed tiger and an email from your boss.
During an acute stress episode, cortisol liberates glucose from the liver so muscles have fuel. Blood pressure rises so oxygen reaches tissue. Digestion and reproduction get temporarily suppressed as non-urgent. Attention sharpens on the immediate threat. When the threat passes, cortisol falls, the parasympathetic nervous system takes over, and repair resumes.
One-time cortisol spikes, even large ones, are not harmful in a healthy person. The body has robust feedback loops that shut off the response within an hour and restore homeostasis. Athletes, public speakers, and emergency workers spike cortisol dozens of times per week without health consequences. The threat is chronic activation, not the individual event.
When acute becomes chronic: how the HPA axis breaks
The HPA axis is built with a self-shutoff mechanism. Cortisol itself signals back to the hypothalamus and pituitary saying: enough, we can stop now. This is called negative feedback, and it is the reason you do not stay in fight-or-flight forever after a single stressful event.
Chronic stress overwhelms that feedback. When cortisol elevation happens for weeks and months rather than hours, the receptors that receive the shutoff signal become less sensitive. The hypothalamus and pituitary stop hearing the message that cortisol is high enough. They keep releasing signals. The adrenals keep releasing cortisol. The rhythm flattens. The morning peak weakens. The evening decline stalls. Levels stay stubbornly elevated even when you feel calm.
This is not adrenal fatigue. That term implies your adrenals get tired and stop making cortisol. The actual research shows the opposite. Under chronic stress, adrenals often produce plenty of cortisol. The failure is upstream in the brain (feedback receptors) and downstream in target tissues (which we come to next). The organ that gets tired is regulation, not production.
·2012·PNASThe mechanism almost no article explains: glucocorticoid receptor resistance
Here is where most cortisol content stops and the real story begins. Every cortisol effect in your body happens because cortisol enters a cell, binds a receptor called the glucocorticoid receptor, and changes which genes get expressed. If that receptor stops responding correctly, high cortisol in the blood produces low cortisol effects in the tissues.
Chronic stress does exactly this. Prolonged glucocorticoid exposure changes the receptors themselves. Some get pulled off the cell surface. Others get their signaling machinery chemically modified. Researchers have documented this molecular reorganization across multiple cell types and stress models.
“Chronic stress leads to impaired HPA axis feedback, glucocorticoid receptor resistance, and paradoxical cortisol dysregulation, fostering a pro-inflammatory state.”
This paradox explains why chronic stress causes systemic inflammation even though cortisol is supposed to suppress inflammation. When receptors resist cortisol, the anti-inflammatory brake fails. NF-kB, a master switch of inflammatory gene expression, stays active. Immune cells produce cytokines that damage tissue. The body burns in slow motion.
The receptor resistance model reframes almost every symptom of chronic stress. The problem is not that you have too much cortisol. The problem is that your cells cannot properly hear the cortisol they have. This is why blood tests can look normal while symptoms are severe, and why cortisol-lowering interventions sometimes disappoint. What has to be restored is receptor sensitivity, not just hormone level.
The seven systems chronic cortisol rewrites
Every symptom of chronic stress traces back to one of two mechanisms already described. Either the HPA axis is stuck in overdrive and cortisol rhythm is flattened, or receptors have grown resistant and tissue effects are miscalibrated. What follows is the map of where those two mechanisms show up as visible symptoms, with a deeper research piece behind each.
Belly fat: cortisol moves fat, it does not just add it
One of the most consistent findings in cortisol research is that chronic elevation redistributes fat storage. Not just adding weight. Moving it. Visceral fat around the abdomen has more glucocorticoid receptors than subcutaneous fat. Under chronic cortisol exposure, fat gets preferentially deposited around the organs rather than the hips or thighs. This is why the classic cortisol body shape is a thicker midsection despite calorie awareness.
The mechanism involves an enzyme called 11-beta-HSD1 that concentrates cortisol inside abdominal fat cells specifically. Even when blood cortisol looks moderate, the local concentration in visceral fat can be four to five times higher. This creates a self-reinforcing loop where the fat itself becomes a cortisol amplifier.
→The redistribution mechanism explainedCortisol Belly Fat: Why Stress Weight Sits Above the NavelThe brain: memory suppression and prefrontal thinning
Three brain regions carry most of the cognitive cost of chronic cortisol. The hippocampus, where memory is encoded and consolidated. The prefrontal cortex, where decisions and impulse control live. The amygdala, where emotional threat is scanned. Chronic cortisol shrinks the first two and enlarges the third.
That structural shift explains the cognitive fingerprint of chronic stress. Words that will not come. Names forgotten. Decisions that feel impossibly heavy. And under it all, an amygdala louder than baseline, scanning for threats that are not there. This is not laziness or aging. It is what elevated glucocorticoids do to neurons over time.
→The cognitive fog decodedCortisol and Brain Fog: How Chronic Stress Rewrites MemorySleep: the 3 AM waking loop
Waking at 3 AM and being unable to fall back asleep is one of the most common and misunderstood chronic stress symptoms. It is not random. It is the CAR firing four hours too early. When cortisol rhythm inverts, the pre-waking rise happens in the middle of the night rather than at dawn. You wake fully alert, wired, and often anxious, because your body thinks it is morning.
This loop is particularly stubborn because sleep deprivation itself raises next-day cortisol. So one bad night sets up worse cortisol timing the following night, which produces another 3 AM wake, and the loop tightens. Breaking it requires simultaneously restoring the evening decline and protecting the deep sleep window.
→The 3 AM mechanismWhy You Wake Up at 3 AM: The Cortisol Sleep Loop ExplainedHormones: cortisol suppresses testosterone, estrogen, and thyroid
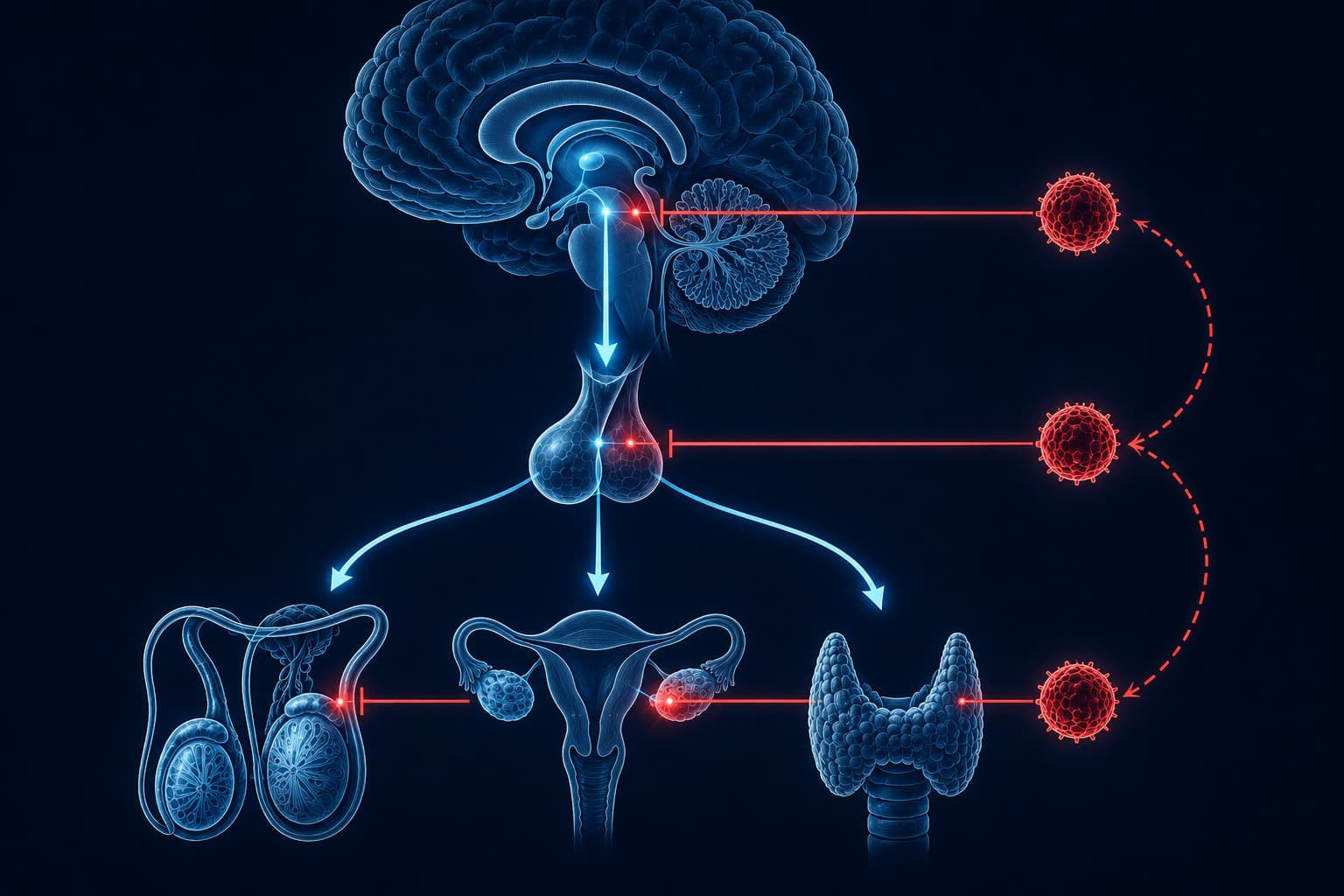
The HPA axis does not exist in isolation. It shares regulatory territory with the HPG axis (which controls reproductive hormones) and the HPT axis (which controls thyroid). Chronic cortisol elevation suppresses all three simultaneously at three levels: hypothalamus, pituitary, and gland.
The clinical picture is predictable once you know the mechanism. Low libido and irregular cycles because gonadotropins, the pituitary hormones that signal your reproductive glands, drop. Fatigue that does not lift with sleep because the conversion of thyroid hormone from its inactive storage form (T4) to its active form (T3) stalls. Free T3 goes down while TSH, the pituitary signal used in standard thyroid panels, stays normal. This is why routine blood work often misses stress-driven hypothyroid symptoms entirely.
→The three-axis suppressionCortisol and Your Other Hormones: How Chronic Stress Suppresses Testosterone, Estrogen, and ThyroidThe immune system: the paradox of getting sick after stress ends
Almost everyone has experienced this. You push through a stressful project, exam, or life transition without catching a cold. The moment it ends, you get sick. This is not coincidence. It is the immune rebound effect.
During the acute phase, cortisol suppresses immune activation. As chronic stress winds down and cortisol falls, previously suppressed immune cells surge back online. Any pathogens that had been quietly replicating in the background now trigger a full response. The illness feels like reward for finishing the hard thing. It is actually the delayed bill.
→The rebound decodedWhy You Get Sick After Stress Ends: The Cortisol Immune ReboundSocial perception: neutral faces read as threat
This one surprises most readers. Chronic cortisol elevation biases how the brain reads other people's faces. Under sustained stress, ambiguous or neutral expressions get interpreted as hostile more often than they would in a calm state. The amygdala shortcut has been re-calibrated toward threat detection.
The relationship consequences are real. Partners feel misread. Coworkers seem judgmental. Social withdrawal starts making sense as protection. What is actually happening is a threat-detection circuit that has stopped receiving the calm-context signal from the prefrontal cortex, because that region is itself under-recruited from chronic stress.
→The threat-perception shiftCortisol and Social Behavior: How Chronic Stress Rewires How You Read PeopleThe order of operations that actually rebalances cortisol
The reason most cortisol-lowering advice fails is that it targets a single lever. Ashwagandha, sleep, exercise, mindfulness, magnesium. Each of these has research behind it. Alone, none of them can restore a broken rhythm because the system has multiple simultaneous failures.
Recovery requires a stacked protocol that addresses the HPA feedback failure, the receptor sensitivity, the circadian rhythm, and the downstream inflammation together. Order matters. Foundation before amplifiers. Rhythm restoration before intensity. Nervous system regulation before adaptogenic support. Doing them in the wrong order is why so many wellness protocols underdeliver.
Morning light exposure and sleep architecture come first because they anchor the circadian rhythm that everything else depends on. Movement and vagal tone come next because they teach the parasympathetic nervous system how to reactivate. Adaptogens and micronutrient support come last because they amplify a system that is already trying to rebalance. Skipping the first two makes the last two feel like they are not working.
What is not cortisol
The wellness industry has built an entire economy on cortisol anxiety. Some of the messaging is accurate. Much of it is not. Three myths dominate the space and understanding them cleans up a lot of confusion.
Common cortisol myths
- Adrenal fatigue causes chronic tiredness
- Cortisol tests can diagnose your stress problem
- Cortisol-lowering supplements fix the underlying issue
- All morning cortisol is bad and should be reduced
- You can biohack your way out of chronic stress with supplements alone
What the research actually shows
- HPA feedback failure and receptor resistance, not adrenal exhaustion
- Cortisol tests miss receptor-level dysfunction entirely
- Supplements amplify recovery but do not initiate it
- The CAR is essential; the goal is a sharp rhythm, not a low peak
- Rhythm restoration requires behavior change first, supplements second
The adrenal fatigue myth persists because it names a real experience (bone-deep exhaustion under chronic stress) with a wrong mechanism. Naming the experience feels validating. The wrong mechanism leads people to expensive supplements aimed at restoring adrenal function when the actual failure is elsewhere. The exhaustion is real. The label is misleading.
Understand every mechanism behind chronic stress
This site publishes research-based deep dives on how cortisol reshapes the body. Subscribe to receive new pieces on the systems chronic stress affects and the protocols that actually restore rhythm.
Get research digestsWhat makes cortisol worth understanding is not that it is dangerous. It is that it sits at the intersection of almost every system in the body. Sleep. Metabolism. Memory. Immunity. Reproduction. Social perception. Get the cortisol rhythm right and every one of those systems has an easier job. Get it wrong and no single intervention downstream can fully compensate.
The mistake to avoid is treating cortisol as a number to lower. The mistake to make instead is treating cortisol as a signal to restore. Your body already knows how to run this system correctly. It ran it correctly for most of your life. Chronic stress teaches the wrong pattern. Recovery is not learning a new pattern. It is remembering the old one, the one your biology was built for, the one that was always available underneath everything you have layered on top.
GetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.