Your hormones don't operate in separate departments. They share a command structure, and when cortisol takes over that structure, it reassigns the budget.
Chronic cortisol elevation systematically suppresses the reproductive and metabolic hormone cascade: reducing GnRH at the hypothalamus, dropping LH and FSH from the pituitary, suppressing testosterone in men, disrupting ovulation and progesterone in women, and impairing the conversion of thyroid hormone into its active form while redirecting T4 toward an inactive blocker. This is not malfunction. It is survival biology operating in a context it was never designed for.
Cortisol does not stop at cortisol. This is what most stress education leaves out. People learn that cortisol rises under stress, that it affects weight and sleep, and that lowering it would help. What they rarely learn is the full architecture: cortisol is produced by a command system called the hypothalamic-pituitary-adrenal axis, and that same system governs every other major hormonal pathway in the body. When it shifts into chronic emergency mode, it does not simply raise cortisol. It reorganizes the entire hormonal budget, redirecting resources from reproduction, metabolism, and growth toward immediate survival. The result is a cluster of symptoms that feel like hormone problems but are, at their root, a stress problem wearing a hormonal disguise.
The Same Axis, the Same Command Structure
The hypothalamus issues two critically important hormonal signals. One is corticotropin-releasing hormone (CRH), which initiates the cortisol stress response. The other is gonadotropin-releasing hormone (GnRH), which drives reproductive hormone production. These two signals operate in inverse relationship: when CRH goes up, GnRH goes down.
The hypothalamus does not run both systems at full capacity simultaneously. It allocates.
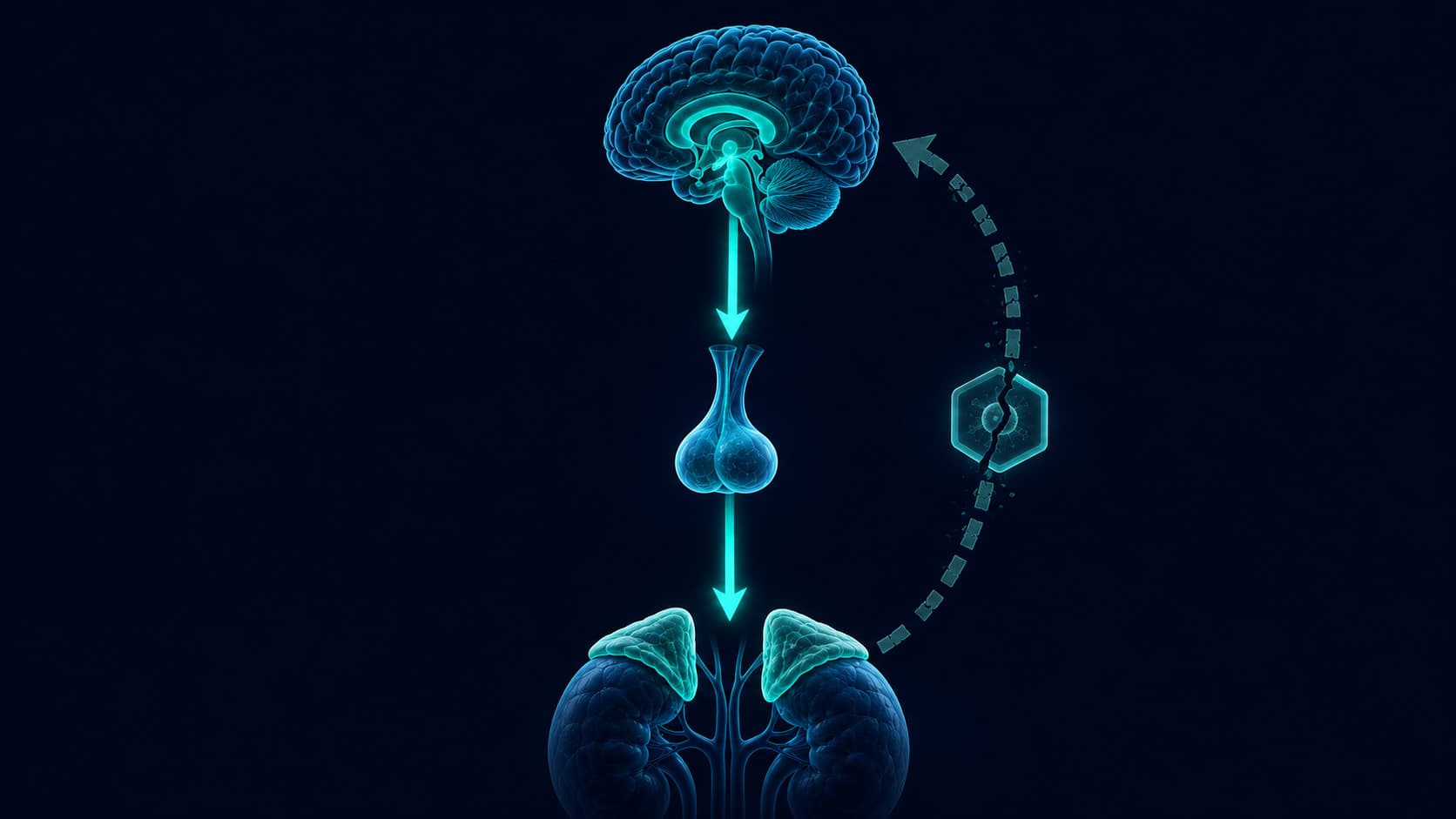
When stress is chronic and CRH remains persistently elevated, GnRH secretion drops. The pituitary receives less GnRH and reduces its output of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH in men drives testosterone production in the testes. LH and FSH in women govern ovulation and the hormonal sequence of the menstrual cycle. Both systems receive less signal. Both produce less.
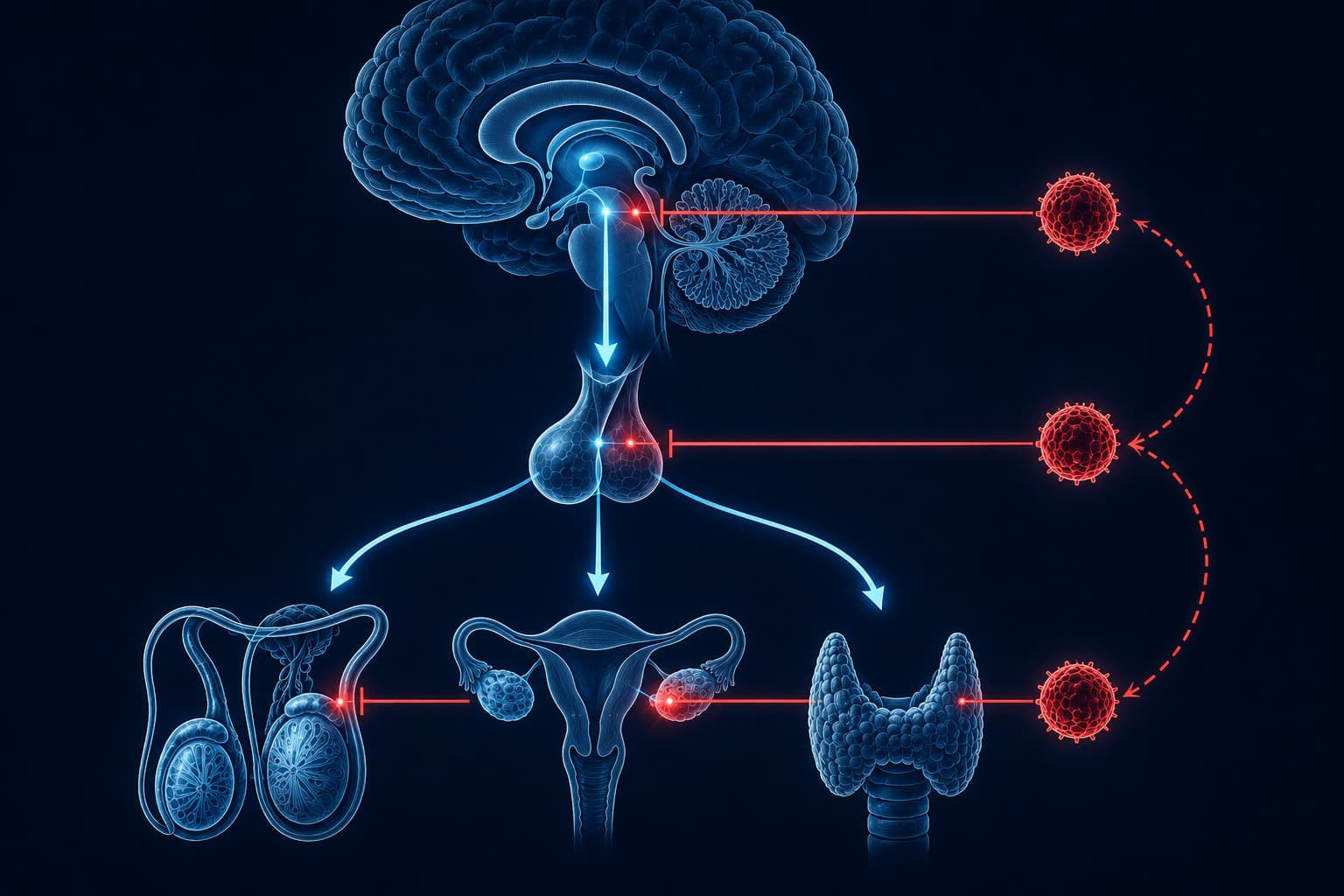
Cortisol then adds a direct second layer. It acts on the pituitary to reduce its sensitivity to whatever GnRH signal does arrive. And it acts directly on the gonads, testes and ovaries, to impair their response to LH. Research in neuroendocrinology set out to characterize exactly how far this interference extended across the reproductive axis.
Research published in Nature Reviews Endocrinology documents glucocorticoid suppression of reproductive function at the hypothalamus (GnRH reduction), the pituitary (gonadotropin suppression), and directly at the gonads (impaired steroidogenesis). The authors note this triple-level suppression reflects the evolutionary priority structure of the stress response: reproduction is a long-term investment, and survival requires its deferral.
This is not one point of failure. It is a coordinated reduction operating simultaneously at every relay point in the system.
Cortisol and testosterone are synthesized from the same precursor molecule. Pregnenolone, produced from cholesterol, is the starting point for both cortisol and sex hormones including testosterone, estrogen, and progesterone. Under chronic stress, the cortisol synthesis pathway is prioritized, diverting this shared substrate away from sex hormone production. When cortisol demand is sustained for months, there is simply less raw material reaching testosterone and estrogen synthesis.
What This Does to Testosterone in Men
The relationship between cortisol and testosterone in men has been studied reliably for decades. Acute psychological stress triggers a measurable testosterone drop within 15 to 30 minutes, mediated partly by direct glucocorticoid action on Leydig cells in the testes. Cumming and colleagues designed a controlled experiment to isolate this effect, administering cortisol to healthy men and measuring the subsequent changes in circulating testosterone levels.
When stress becomes chronic, the effect shifts from episodic suppression to baseline recalibration. The hypothalamic-pituitary-testicular axis does not simply dip and recover. It adjusts its operating setpoint downward. Men under sustained occupational or psychological stress consistently show lower morning testosterone, reduced LH pulsatility, and diminished testicular response to hormonal signals, even after controlling for age, sleep quality, and body composition.
The lived experience is recognizable: diminished libido, slower recovery from training, reduced muscle response, mood instability, and a quality of mental flatness that does not quite resemble depression but feels close enough to be confusing.
These are not character failures or signs of aging. They are the predictable outputs of a hormonal system that has been running in emergency mode long enough to forget what its baseline felt like.
There is a further dimension most discussions miss. The adrenal glands produce both cortisol and DHEA-S (dehydroepiandrosterone sulfate), an androgen precursor that serves as a reserve buffer for testosterone synthesis. Under chronic stress, adrenal output shifts progressively toward cortisol and away from DHEA-S. As this buffer depletes, the substrate competition that cortisol already creates loses its natural partial counterbalance. Researchers studying HPA axis dysregulation increasingly track the cortisol-to-DHEA-S ratio as a more sensitive marker of this shift than either hormone measured in isolation. A rising ratio reflects an adrenal system that has fully committed to survival at the expense of anabolic function.

“The data indicate that cortisol has a direct inhibitory effect on circulating testosterone levels.”
What This Does to Women: Cycles, Ovulation, and the Progesterone Problem
In women, the hormonal consequences of chronic cortisol are more complex because the menstrual cycle is not a single hormone. It is a monthly sequence. Cortisol can disrupt it at multiple points.
The most consistently documented effect is disruption of the luteal phase, the post-ovulation period during which progesterone rises and prepares the uterine lining. Cortisol and progesterone compete for the same receptors. Elevated cortisol can functionally block progesterone signaling even when blood progesterone levels appear normal on a test. The outcome is premenstrual symptoms: irritability, water retention, disrupted sleep, heightened anxiety. These reflect a cortisol-driven reduction in progesterone's functional effect, not a deficiency in its production.
In higher-stress periods, ovulation itself may be suppressed or delayed. The hypothalamus, responding to elevated CRH, reduces GnRH pulsatility, which means the LH surge that triggers ovulation may not occur on schedule, or at all. Cycles lengthen. Periods are missed. Anovulatory cycles emerge in which menstruation occurs without ovulation. This pattern is frequently attributed to unrelated gynecological causes rather than to the upstream cortisol mechanism driving it.
The suppression begins earlier than most people expect. CRH inhibits GnRH through two simultaneous pathways. One is direct: CRH acts on GnRH neurons and reduces their pulsatile output. The second operates through beta-endorphin, an endogenous opioid that CRH triggers and that independently suppresses GnRH via its own receptor pathway. Both channels run in parallel from the first moments of the stress response. This dual mechanism explains a pattern reported consistently in the research: cycle disruption that appears faster than the cortisol timeline would predict, because the reproductive brake is being applied before cortisol levels have had time to fully elevate.

“Both the chronic administration of glucocorticoids and psychogenic stress are able to inhibit LH secretion through an action at the hypothalamus and pituitary.”
The Thyroid Mechanism Most Stress Discussions Never Reach
The thyroid adds a third dimension to the cortisol cascade. And it is the one most consistently absent from conversations about stress and hormones.
The thyroid produces primarily T4, an inactive form of thyroid hormone that must be converted to T3, the biologically active form, by deiodinase enzymes in peripheral tissues. Cortisol impairs this conversion step. The result is a state in which thyroid hormone is circulating but not fully activating target tissues.
Standard thyroid panels measure TSH and T4. Neither measures T3 or the efficiency of the conversion step that cortisol is impairing. A person under chronic stress can show completely normal TSH and T4 values while experiencing every recognizable symptom of thyroid underfunction: cold extremities, low energy, difficulty losing weight, brain fog, flat mood, reduced motivation.
The labs look fine. The mechanism is not being measured.
There is a second layer. Cortisol does not simply slow T3 production. By upregulating an enzyme class called type 3 deiodinase (D3), it also accelerates the conversion of T4 into reverse T3 (rT3), a mirror-image molecule with the same structure as active T3, but rotated in three-dimensional space. Reverse T3 fits into thyroid hormone receptors the wrong way round. It occupies them without activating them, and while doing so it physically blocks active T3 from binding. The result is not merely less T3 being produced. It is the T3 that does exist being locked out of the sites where it would act.
Reverse T3 is structurally identical to active T3: same atoms, same bonds. The difference is geometry. Its iodine atoms are positioned as a mirror image, causing it to fit into thyroid receptors upside down. It slots in, activates nothing, and prevents active T3 from taking its place. Under chronic cortisol elevation, the body is simultaneously producing less T3 and filling the lock with a key that does not turn.
TSH and T4 do not capture T4-to-T3 conversion efficiency, free T3 levels, or reverse T3. A person can show completely normal TSH and T4 while free T3 is low and rT3 is elevated, producing full thyroid symptom load with no diagnosable thyroid disorder. The complete picture requires free T3 and reverse T3 measured together. If thyroid symptoms are present during a period of high chronic stress, this is the panel to request before assuming a primary thyroid condition.
Why Your Body Does This — and Why It Becomes a Problem
The suppression of testosterone, estrogen, progesterone, and thyroid activity under stress is not a flaw. It is the body allocating resources toward immediate survival at the expense of long-term investment. Reproduction is metabolically expensive. Active thyroid hormone raises metabolic rate and oxygen consumption. Growth requires sustained anabolic signaling.
When a genuine short-term threat demands all available energy, redirecting those resources makes sense.
The design assumes the threat ends. An acute stress response that suppresses reproductive function for 48 hours is adaptive. A chronic stress state that sustains this suppression for months or years was never part of the evolutionary specification. The biology evolved for threats that resolved. Financial pressure, relational conflict, occupational overload: none of these resolve on any timescale the body knows how to read.
Acute stress (hours to days)
- Testosterone drops transiently, recovers with resolution
- Ovulation delayed by days, cycle returns to rhythm
- T3 conversion briefly impaired, normalizes within days
- No lasting setpoint change in the HPG axis
- Body retains a clear memory of its hormonal baseline
Chronic stress (months to years)
- Testosterone baseline recalibrated downward across weeks
- Cycles regularly disrupted, anovulatory patterns emerging
- T3 suppressed, rT3 elevated, receptor blockade structural
- HPG axis setpoint shifts, baseline becomes harder to locate
- Recovery requires deliberate intervention over months
The Loop That Self-Amplifies
The hormonal suppression that chronic cortisol produces is not static.
It feeds back. Low testosterone in men increases cortisol reactivity, reducing the body's capacity to modulate future stress. Low progesterone worsens sleep architecture, which independently elevates the following morning's cortisol. Reduced T3 lowers overall energy output, making existing demands feel heavier than they are. Depleted DHEA-S removes the androgen buffer that partially offset the cortisol effect in the first place. Each deficit created by chronic cortisol makes the stress state harder to exit.
People emerging from burnout frequently report feeling worse in weeks two and three than they did at the peak. The cortisol is dropping. The downstream hormonal systems it suppressed have not yet rebuilt. This is not regression. It is the sequence the research predicts.
What Recovery Actually Looks Like
Cortisol begins to normalize as the primary stressor is managed or removed. CRH pulsatility resets. The hypothalamus begins cautiously re-enabling GnRH secretion.
LH and FSH levels begin recovering. Testosterone in men shows measurable improvement. Menstrual regularity starts returning in women who experienced disruption. T3 conversion improves as cortisol competition with deiodinase enzymes reduces and rT3 levels begin to normalize.
Testosterone continues recovering toward individual baseline. Cycle regularity stabilizes. DHEA-S levels begin rebuilding. Energy and metabolic function improve as T3 reaches functional levels and rT3 receptor competition decreases.
Full hormonal baseline recovery for most individuals without pre-existing deficiencies. The body re-establishes its setpoint. What felt like a permanent state turns out to have been a prolonged suppression.
These timelines assume the primary intervention is addressing the source of chronic stress, not supplementing hormones as the first response. Beginning with testosterone replacement or thyroid medication before addressing cortisol is treating the shadow without removing what is casting it.
The intervention order matters
Hormonal symptoms driven by chronic cortisol often respond poorly to hormonal intervention alone when the upstream suppression remains active. The sequence that research supports: address sleep quality first, then reduce the primary stressor, then support HPA axis recovery, and only then reassess hormonal status with targeted testing before adding any supplementation.
High impactWhich labs to request — and which ones give an incomplete picture
Standard hormone panels miss most of what chronic cortisol is doing. Five variables together provide a complete view: morning cortisol, DHEA-S, free testosterone (not only total), free T3, and reverse T3. The cortisol-to-DHEA-S ratio reveals how far the adrenal system has shifted toward survival. The free T3-to-rT3 ratio reveals whether conversion has been redirected toward the inactive form. Neither picture appears on a routine panel.
High impact“Glucocorticoids have inhibitory effects on reproductive function at multiple levels of the hypothalamic-pituitary-gonadal axis, as well as directly on the gonads themselves.”
“Glucocorticoids also inhibit the secretion of GnRH from the hypothalamus, thereby reducing gonadotropin secretion and, ultimately, gonadal steroid levels.”
“Type 3 deiodinase activity is upregulated under conditions of physiological stress, diverting T4 conversion toward reverse T3 and reducing the availability of active T3 in peripheral tissues.”
Get the Full Cortisol Series
This is Article 5 of the GetClariSync cortisol series. Previous pieces cover what cortisol actually does, how it redistributes fat to the abdomen, how it erodes memory and focus, and why it wakes you at 3AM.
Explore the Body CategoryGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.