Over 800 million TikTok views on cortisol detox. A wave of home saliva tests. Products promising to purge a hormone that cannot be purged. Endocrinologists have a clear verdict on most of it. Here is what the research actually shows, and the order in which it works.
Chronic HPA axis dysregulation is not primarily a problem of cortisol overproduction. It is a problem of impaired negative feedback: glucocorticoid receptors in the hippocampus desensitize under sustained cortisol exposure, and the axis loses its ability to self-terminate stress responses. Recovery targets receptor re-sensitization and diurnal rhythm restoration, not cortisol suppression. The protocol has six layers, each addressing a distinct biological repair point, and the sequence matters: foundational layers must be established before later ones produce their intended effect. Timeline: 6 to 16 weeks.
The cortisol detox trend is built on a fundamental misreading of physiology. Cortisol is not a toxin. It is not stored in tissue. It cannot be cleansed, purged, or drained. It is a hormone produced continuously by the adrenal cortex in response to signals from the brain, and the brain-adrenal feedback loop runs every moment of every day. What breaks down in chronic stress is not that the system produces too much cortisol. What breaks down is that the system loses the ability to tell itself to stop.
The Real Problem: The Brake System Stopped Working
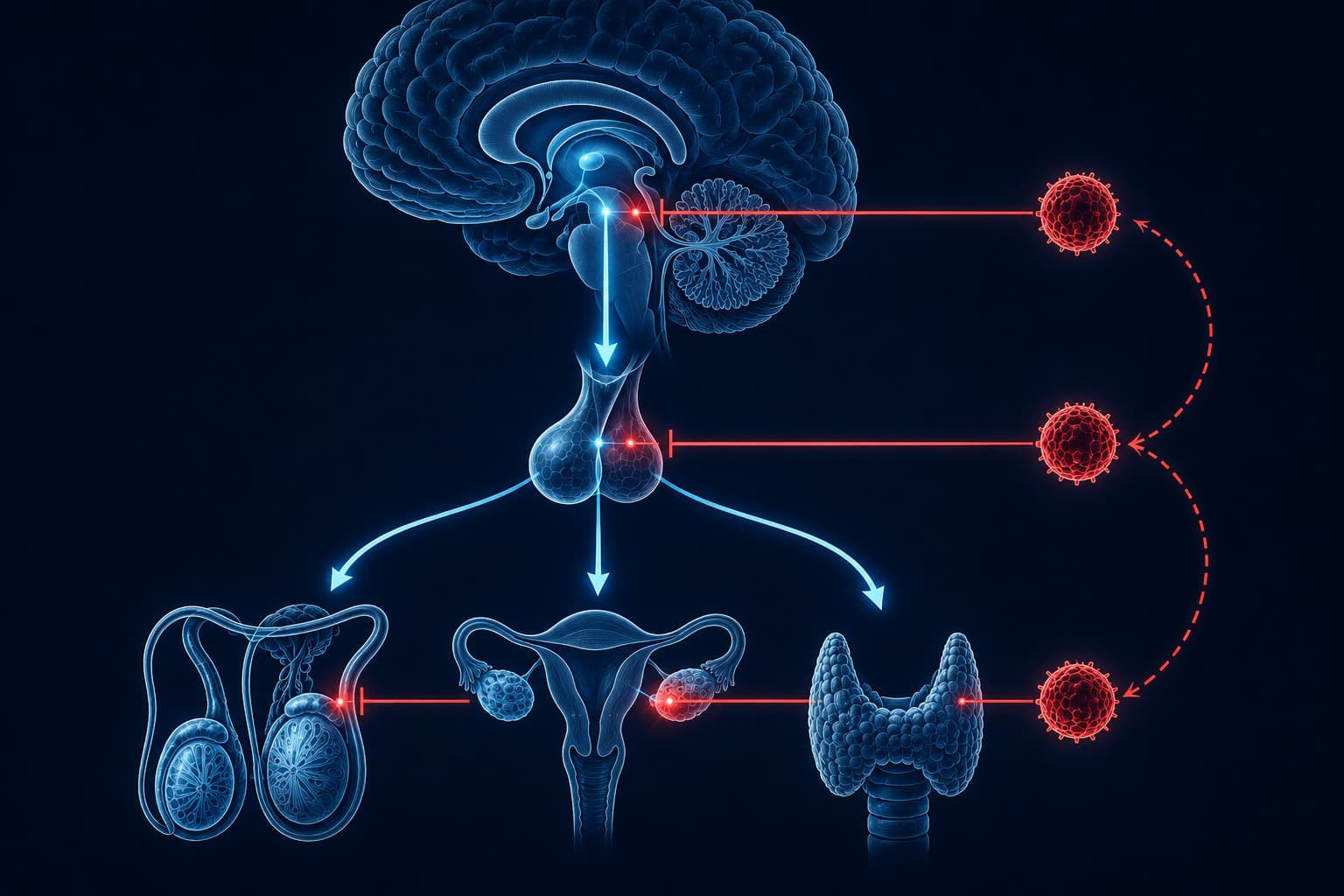
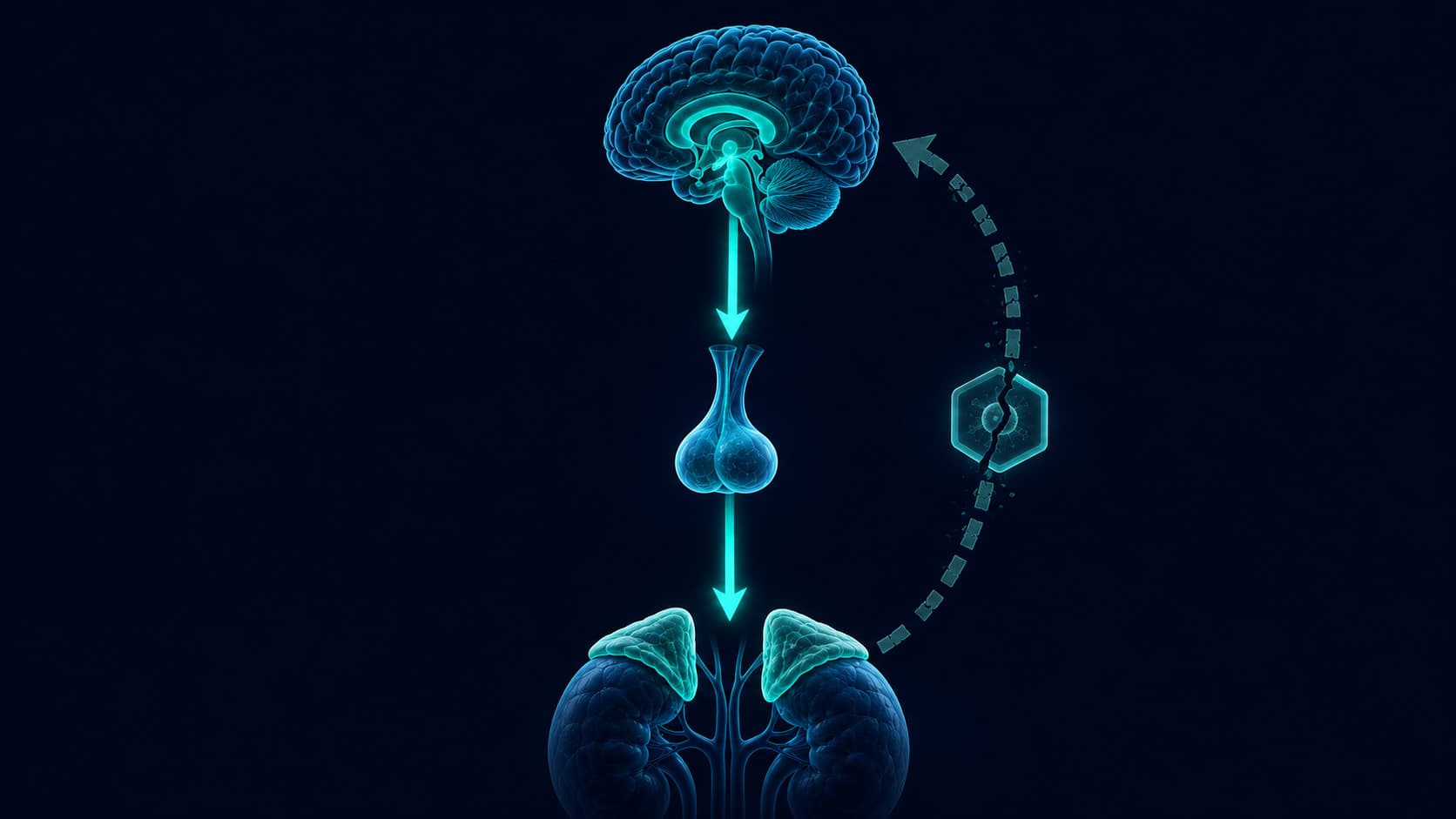
The HPA axis self-regulates through negative feedback. When cortisol rises, it binds to glucocorticoid receptors (GRs) in the hippocampus and prefrontal cortex. These structures signal back to the hypothalamus to reduce CRH output, which reduces ACTH, which reduces cortisol production. The loop closes. The stress response terminates.
Under chronic elevation, something changes. Sustained cortisol exposure desensitizes and downregulates GR expression in the hippocampus, damaging the structure responsible for the shutdown signal. The axis cannot close the loop. Cortisol stays elevated not because the adrenals are in overdrive, but because the feedback pathway is no longer functional. The problem is the brake, not the accelerator.
A 2025 integrative review identifies glucocorticoid receptor sensitivity as the central variable in HPA axis recovery. Interventions that restore hippocampal GR expression and negative feedback efficiency produce lasting recalibration. Those that simply suppress cortisol output do not. The review specifies that recovery requires a multifactorial protocol: sleep restoration, exercise adaptation, nutritional correction, and psychological stress reduction. No single intervention is sufficient alone.
This reframe changes what recovery looks like. The goal is not to drive cortisol to a lower number on a lab panel. The goal is to restore the system's capacity to regulate itself. An axis that can mount and cleanly terminate a cortisol response is a healthy axis. An axis that mounts responses easily and cannot terminate them is the pathological one, regardless of what a single cortisol reading shows.
The Protocol Is a Stack, Not a Menu
Every mainstream article on cortisol reduction presents its recommendations as interchangeable options. Meditation, ashwagandha, cold showers, exercise, sleep — as if the reader should pick three and rotate through them. The biology does not work this way. Some interventions operate at the foundational level: without them, nothing else functions properly. Others are finishing layers: effective only once the foundation is established. Applying them out of order explains why so many people feel like nothing is working.
The six layers below are ordered by mechanistic priority. Each one builds on what precedes it.
Layer 1: Re-anchor the Diurnal Rhythm With Morning Light
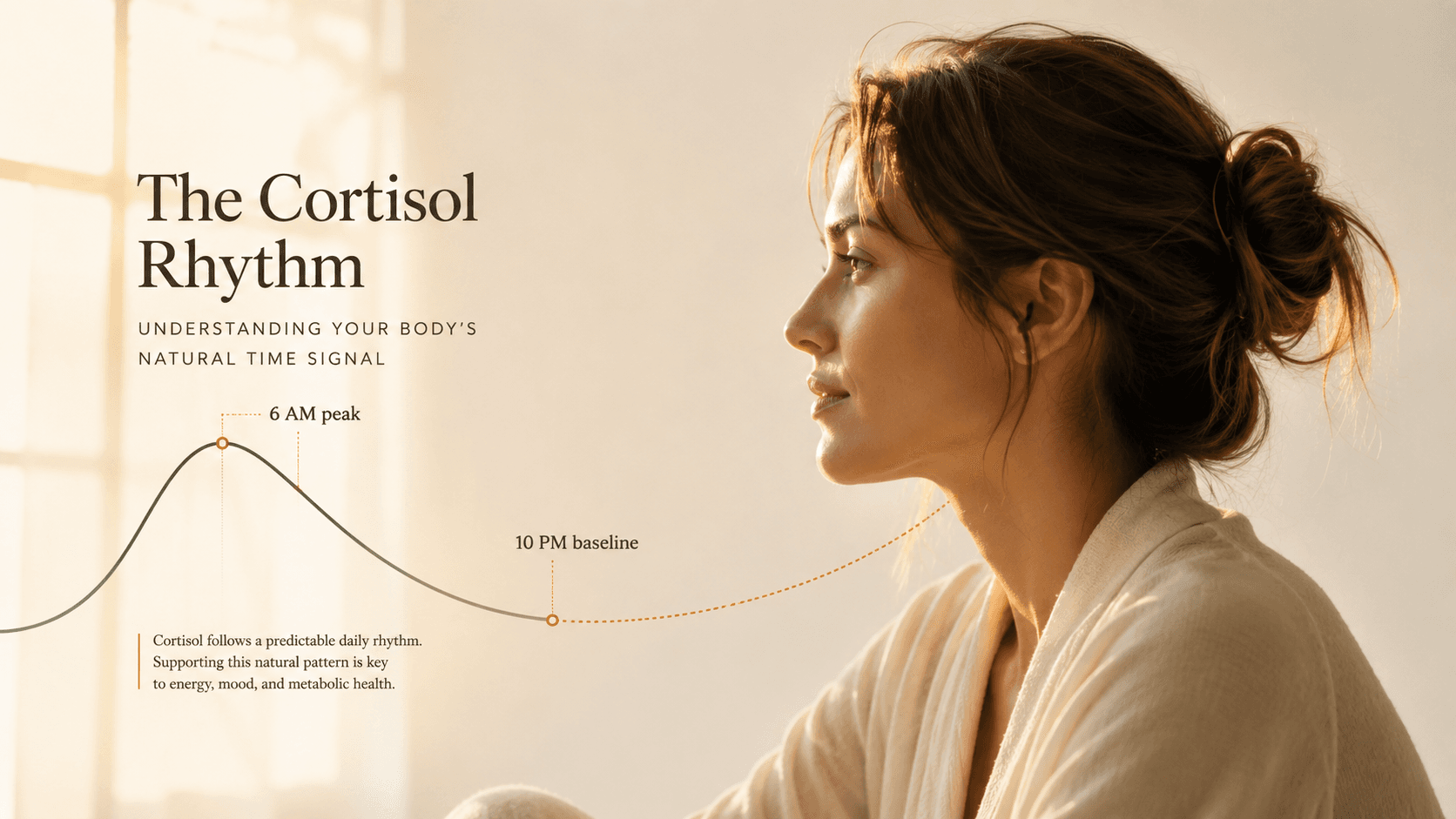
The HPA axis does not operate at a constant level throughout the day. It follows a diurnal rhythm: a sharp peak within 30 to 45 minutes of waking, a steep morning-to-afternoon decline, and a near-zero trough at midnight. This rhythm is synchronized by the suprachiasmatic nucleus (SCN) in the hypothalamus, which receives its primary input from the retina. Specifically, from short-wavelength blue-green light in the early morning hours.
In a chronically dysregulated system, this diurnal slope flattens. Cortisol does not peak cleanly in the morning, or peaks at the wrong point in the day. Morning bright light exposure is the most direct mechanism for restoring it. It amplifies the cortisol awakening response (CAR), sets the SCN oscillator for the next 24 hours, and pulls the downstream hormonal rhythm back into alignment. Nothing else in the protocol performs this function. It must come first.

Morning light: the practical protocol
10 to 30 minutes of outdoor light exposure within 60 minutes of waking. An overcast sky still delivers 10,000 lux, roughly 50 times more than indoor lighting. No sunglasses during this window; the blue-green signal must reach the retina. Winter at northern latitudes: a 10,000-lux light therapy lamp at 30 cm for 20 minutes produces a comparable effect. This is the only intervention in the protocol that cannot be substituted. It anchors the rhythm that makes every subsequent layer more effective.
High impact“Bright morning light significantly elevated cortisol versus dim light controls, with the effect mediated through short-wavelength retinal stimulation of the SCN-HPA axis pathway. Irregular light exposure was associated with flattened diurnal cortisol slopes.”
Layer 2: Protect the Sleep Architecture That Suppresses the Axis Overnight
Sleep does not reduce cortisol simply by providing rest. Specific sleep stages actively suppress the HPA axis through distinct mechanisms. Slow-wave sleep (SWS, deep non-REM sleep) is significantly coupled to declining plasma cortisol. During SWS episodes, the axis is actively inhibited. Disruption of SWS, through alcohol, late exercise, inconsistent timing, or evening light exposure, removes the overnight suppression on which the entire recovery depends.
The relationship is bidirectional and self-reinforcing in the wrong direction: elevated nocturnal cortisol suppresses SWS, which prevents HPA recalibration, which keeps nocturnal cortisol elevated. For recovery purposes, sleep architecture matters more than total sleep hours. Eight hours of fragmented, SWS-depleted sleep provides less HPA suppression than six hours of consolidated, architecturally intact sleep.
- Alcohol within 3 hours of sleep: suppresses SWS in the first half of the night
- Intense exercise within 3 hours of bedtime: elevates cortisol during its natural declining window
- Eating within 2 hours of sleep: activates digestive-insulin signaling, fragments SWS architecture
- Inconsistent sleep timing: shifts circadian phase, misaligns SWS occurrence with peak suppression window
- Screen light after 9pm: delays melatonin onset, compresses early SWS episodes
“Sleep restriction was followed by elevated cortisol concentrations the next evening, reflecting impaired HPA negative feedback the morning after sleep loss, a finding consistent with GR desensitization under sleep deprivation conditions.”
Layer 3: Correct the Magnesium Floor
Magnesium occupies an unusual position in this protocol: it does not support HPA recovery, it determines the system's baseline sensitivity. Magnesium deficiency increases CRH transcription in the paraventricular nucleus of the hypothalamus — the structure that initiates the cortisol cascade. A magnesium-deficient individual has a structurally elevated HPA set-point. Behavioral interventions reduce stress reactions from that elevated set-point. They do not lower the set-point itself.
The loop reinforces in both directions: magnesium deficiency raises cortisol output, and elevated cortisol promotes urinary magnesium excretion. A person under sustained stress actively depletes the mineral that would otherwise blunt their stress response.
Dietary magnesium from leafy greens, seeds, and legumes is the preferred source. Supplemental forms with better absorption evidence: magnesium glycinate and malate for general use, magnesium L-threonate for central nervous system penetration. Research dosing: 200 to 400 mg elemental magnesium. Magnesium oxide has poor bioavailability and accounts for most of the reports that magnesium supplementation did nothing.
“A deficit in magnesium increases susceptibility to stress, while stress increases renal excretion of magnesium, generating a self-reinforcing loop that maintains HPA hyperactivation independent of the primary stressor.”
Layer 4: Use Exercise as Inoculation, Not Avoidance
Exercise acutely spikes cortisol. This is not a side effect. It is the mechanism. The HPA response to a moderate session trains the negative feedback loop by requiring it to mount a controlled response and then cleanly terminate it. Repeated practice of this cycle improves the termination speed and efficiency of the feedback pathway, which is precisely what chronic stress has degraded. The spike is the point.
A 2026 preprint examined what happens in CRH-expressing neurons of the paraventricular nucleus when exercise follows a psychological stressor rather than precedes it, tracking BDNF and corticosterone interactions across both sequences.

Exercise immediately following a psychological stressor elevated both corticosterone and hypothalamic BDNF. Their synergistic action in CRH-expressing PVN neurons reversed behavioral sensitization and synaptic metaplasticity induced by the stressor. The effect was not observed when exercise preceded the stressor. This is preliminary data from a preprint — replication in peer-reviewed trials is needed before clinical application.
“Exercise performed after a stressor, but not before, leverages a therapeutic window in CRH neurons involving BDNF-corticosterone synergy that reverses stress-induced behavioral sensitization and synaptic metaplasticity.”
The window is time-sensitive: exercise must follow the stressor, not precede it. For recovery from an acutely stressful event, a post-stressor session may be the more targeted intervention, the opposite of conventional advice to exercise before a difficult day.
Layer 5: Activate the Vagal Brake Directly
The vagus nerve and the HPA axis are in a bidirectional relationship. Vagal tone inversely predicts HPA reactivity: higher resting heart rate variability (HRV) is associated with attenuated cortisol responses to stressors. Interventions that directly increase vagal output suppress HPA activation through the same feedback architecture that the axis itself uses.
Slow-paced breathing at 6 breaths per minute maximizes respiratory sinus arrhythmia and produces the largest documented acute increases in vagal tone. This is not a relaxation technique in the casual sense. It is a direct physiological input to the autonomic system that measurably shifts balance from sympathetic to parasympathetic dominance. The cortisol effect is downstream of this shift, not immediate; consistent daily practice over weeks produces the HPA adaptation.
Resonance Frequency Breathing (6 breaths/min)
Nature exposure operates on overlapping mechanisms. A 2019 meta-analysis screened 971 studies to examine whether forest and natural environments produce measurable salivary cortisol changes compared to urban controls, incorporating both pre- and post-intervention measurement points.
“Forest bathing significantly reduced salivary cortisol concentrations compared to urban control conditions, with the effect observed consistently across pre- and post-intervention time points in 22 included studies.”
The mechanisms include reduced visual and auditory threat stimuli, attentional restoration, and direct parasympathetic activation. A forest is not required: any low-stimulation outdoor environment with natural features produces a measurable effect.
Layer 6: Adaptive Support (After the Foundation, Not Instead of It)
Ashwagandha and phosphatidylserine are the two supplements with the strongest evidence for cortisol modulation. Neither replaces the protocol that precedes them. Both blunt acute cortisol peaks and attenuate HPA reactivity to stressors, but they do not restore GR sensitivity, recalibrate the diurnal rhythm, or compensate for disrupted sleep architecture. Their typical failure mode is being used first, alone, without any foundational layer in place.
Evidence-supported
- Ashwagandha KSM-66 (300–600 mg/day): 22–28% serum cortisol reduction in 60-day RCTs, via HPA reactivity attenuation
- Phosphatidylserine (400–800 mg/day): blunts exercise- and stress-induced cortisol peaks without suppressing basal rhythm
- Magnesium glycinate/malate (200–400 mg elemental): corrects HPA set-point elevation from deficiency
- Omega-3 fatty acids (2.5g DHA+EPA/day): modest HPA reactivity reduction in 3-week RCTs
Insufficient or no evidence
- Cortisol detox products: no mechanism for cortisol removal; cortisol is not stored in tissue
- Home saliva cortisol tests: extreme diurnal variation makes single-point testing clinically unreliable
- Cold water immersion as primary intervention: acute cortisol spike normalizes within 1 hour; long-term HPA evidence remains modest
- Rhodiola without foundational protocol: adaptogen effects modest; no verified HPA mechanistic evidence at therapeutic doses
“The ashwagandha group showed a significant reduction in serum cortisol (27.9% vs 7.9% in placebo) along with improvement in all stress and anxiety measures at 60 days, suggesting HPA reactivity attenuation as the primary mechanism.”
The Oldest Cortisol Suppression System in the Brain
Before any of the above interventions were studied, mammals had a cortisol regulation mechanism that predates the modern HPA axis in evolutionary time: social bonding. Oxytocin, the neuropeptide released during physical closeness and trusted social contact, directly inhibits HPA axis activity. Heinrichs and colleagues designed a controlled study to test whether social support and oxytocin produced additive cortisol effects, administering oxytocin intranasally across conditions with and without in-person social support present, then measuring responses to a standardized stress protocol.
The effect requires physical presence. Phone calls, text messages, and social media contact do not produce the same oxytocin-mediated HPA suppression. The mechanism operates on proximity, touch, and facial signal exchange — inputs that digital communication cannot replicate.
“Oxytocin and social support interacted to produce the lowest cortisol and subjective stress levels. Neither condition alone produced an equivalent effect, indicating that physical social presence is required to potentiate the oxytocin-HPA suppression mechanism.”
What the Timeline Actually Looks Like
Realistic recovery from HPA dysregulation is measured in weeks and months. GR receptor re-sensitization, hippocampal structural recovery, oxytocin receptor upregulation, and circadian rhythm recalibration each operate on their own biological timeline. None respond to days of effort. The typical trajectory across mechanisms in the research literature:
Morning light and sleep consistency begin anchoring the diurnal rhythm. CAR amplitude starts recovering. Irritability from acute cortisol fluctuation begins reducing. Magnesium correction starts addressing the set-point deficit.
SWS architecture improves with consistent sleep timing and evening protocol. Nocturnal cortisol begins declining. Ashwagandha (added in week 2–3) shows initial HPA reactivity attenuation. Exercise feedback loop adaptation becomes measurable.
Diurnal slope steepens toward a normal shape: robust CAR, afternoon decline, low midnight reading. GR sensitivity begins recovering in hippocampus. Consistent in-person social contact measurably suppresses HPA reactivity to acute stressors.
Full diurnal rhythm recalibration in most cases without additional chronic stressors. HPA negative feedback efficiency approaching baseline. The axis mounts responses and terminates them cleanly. This — a functional rhythm, not a single cortisol number — is the marker of recovery.
The axis that got here under sustained pressure will not reset under more pressure. The protocol is slow, layered, and non-negotiable about its sequence. In every mechanism we have studied, it is also reversible.
“HPA axis recovery requires a multifactorial approach targeting glucocorticoid receptor sensitivity, sleep restoration, physical activity adaptation, and nutritional correction simultaneously. No single intervention has demonstrated sufficient efficacy in isolation.”
This completes the cortisol series
Seven articles. One hormone. The full picture: what cortisol does, what it damages, and how the system recovers. Subscribe to receive the next GetClariSync deep dive when it publishes.
Get the newsletterGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.