Your stress has been lower lately. You have been working on it. And you still wake up at 3 AM, wide awake, heart already beating slightly faster, mind already running. The problem is no longer what you think it is.
Chronic stress shifts the Cortisol Awakening Response earlier in the night, producing a cortisol surge between 2 and 4 AM that triggers waking before sleep is complete. Cortisol and melatonin are direct hormonal antagonists — elevated evening cortisol suppresses melatonin onset, while poor sleep elevates the following day's cortisol through hippocampal feedback failure. The result is a self-sustaining loop that continues running weeks after the original stressor has resolved.
The person who wakes at 3 AM is often not someone who cannot fall asleep. They fall asleep fine. Sometimes quickly. Then something pulls them out at a specific hour — thoughts already assembled, body already alert, the mind running at a speed that suggests it never actually stopped. This pattern is not random and it is not insomnia in the way most people understand the word. It is the signature of a cortisol clock that has been reset — and a feedback loop between cortisol and sleep that, once established, does not require the original stressor to keep running.
Cortisol and Melatonin Cannot Rise at the Same Time
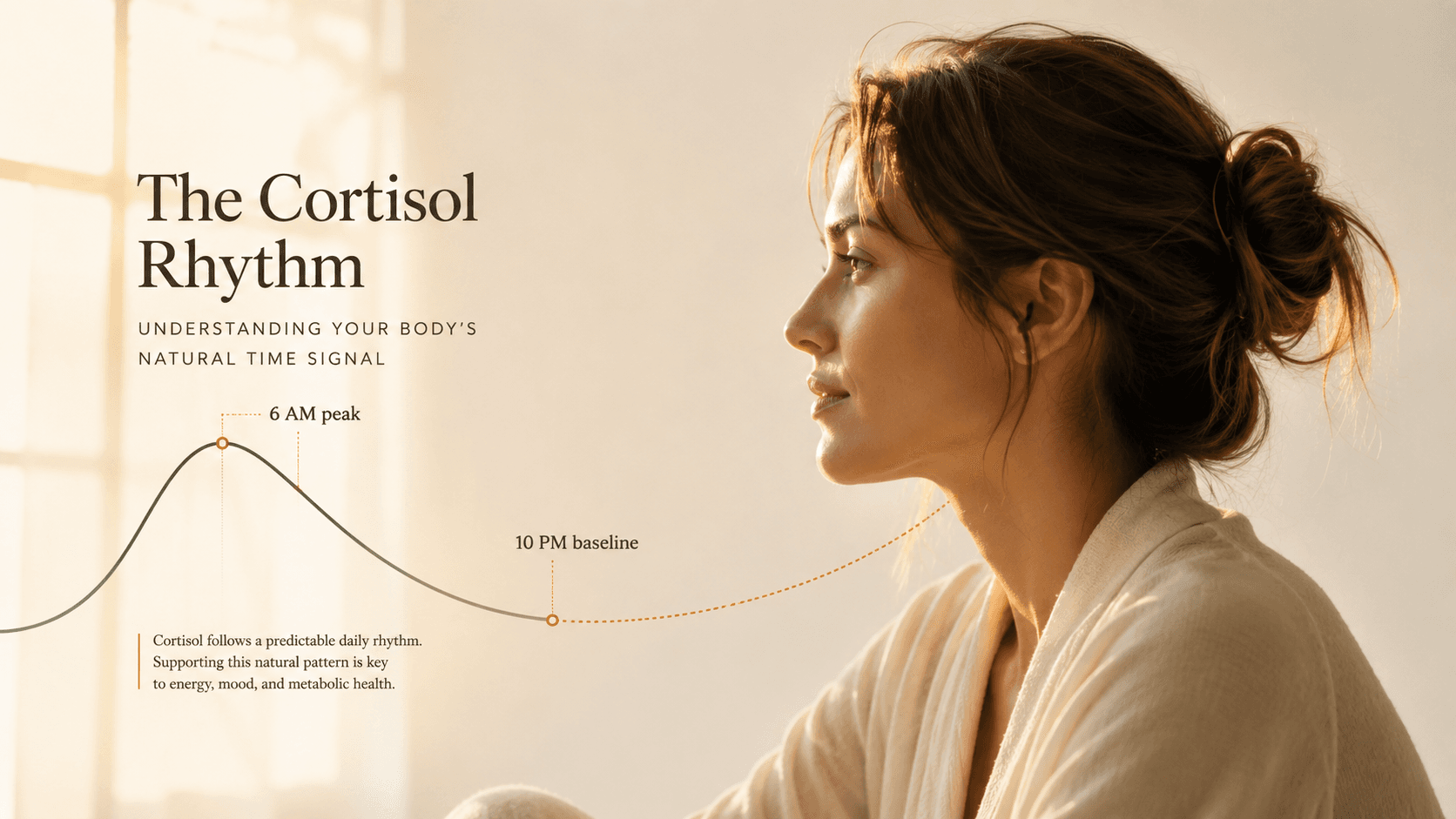
The simplest version of why chronic stress disrupts sleep: cortisol and melatonin are hormonal antagonists. As one rises, the other falls — not as a metaphor for feeling alert, but through direct suppression at the hypothalamic level. A healthy circadian rhythm has cortisol peaking between 7 and 9 AM and reaching its lowest point around midnight. Melatonin does the inverse, rising in the evening as cortisol clears and declining with the morning light signal.
Chronic stress disrupts this by sustaining cortisol elevation into the evening hours when it should be approaching its nadir. The hypothalamus reads elevated cortisol as a 'daytime alert state' signal and delays melatonin secretion accordingly. Melatonin cannot rise when cortisol is still up. The body's chemical trigger for sleep onset simply does not arrive on schedule.
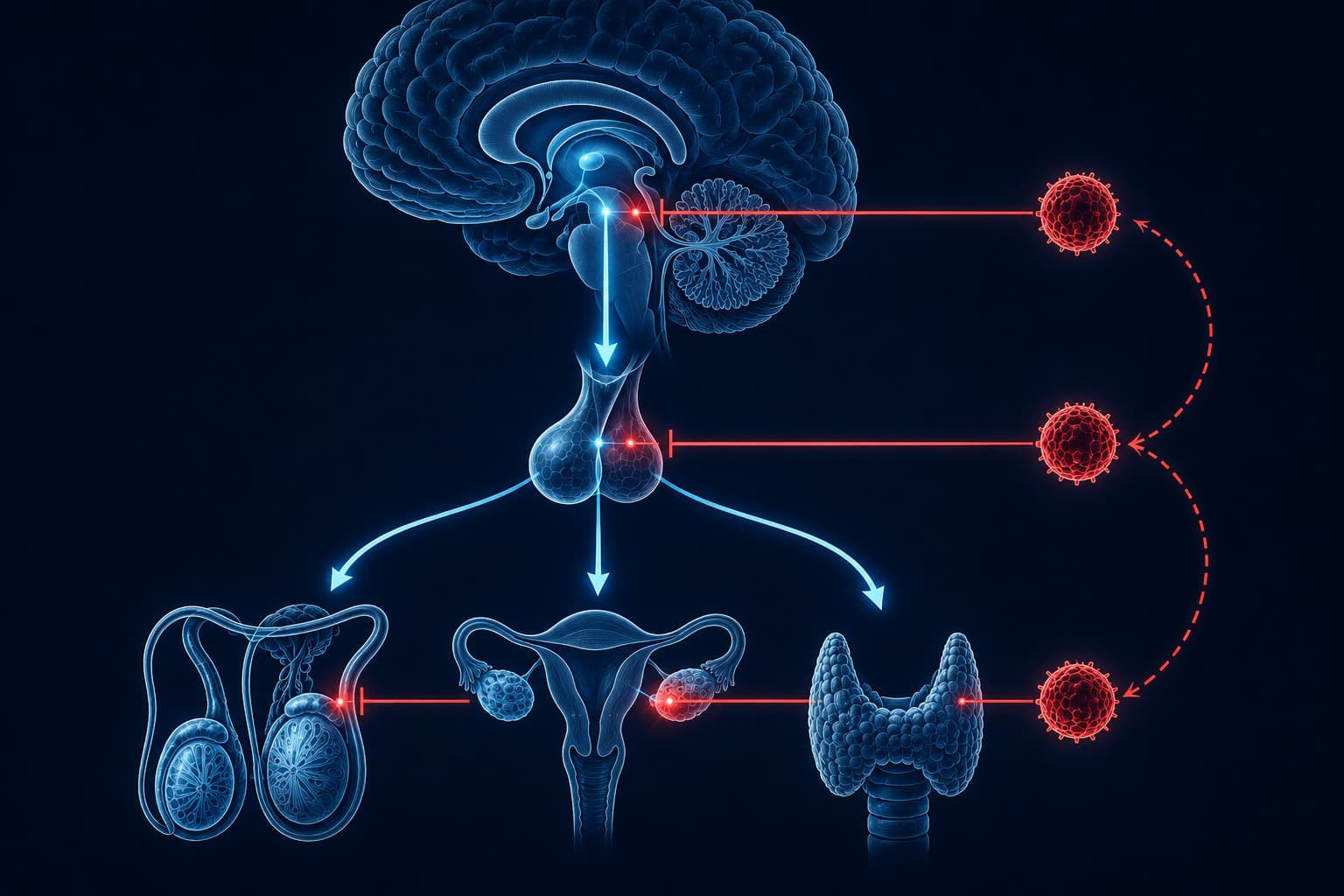
Research on HPA axis and sleep interactions establishes that cortisol and sleep architecture regulate each other in both directions. Elevated cortisol in the first half of the night suppresses slow-wave sleep, while slow-wave sleep itself normally suppresses HPA axis activity. When evening cortisol is chronically elevated, this mutual regulation breaks down: less SWS means less HPA suppression overnight, which means more cortisol the following evening, which means less SWS. The cycle tightens with each repetition.
What this produces over weeks is not insomnia in the clinical sense. It is a systematically degraded sleep architecture in which the most restorative phases are specifically impaired while the body retains enough function to fall asleep and maintain lighter stages. You sleep. The sleep does not do what sleep is supposed to do.
Why 3 AM Is Not a Random Hour
In healthy adults, cortisol begins rising approximately 20 to 30 minutes before anticipated wake time, peaking between 30 and 45 minutes after waking. This is the Cortisol Awakening Response — a biological preparation signal that mobilizes glucose, activates immune surveillance, and primes cognitive function for the day ahead. It is tightly calibrated to anticipated wake time, not to sunrise.
Chronic stress amplifies and destabilizes this response. Research consistently documents that people under sustained high-stress conditions show an exaggerated and earlier CAR — the morning cortisol surge begins before its scheduled time. When this shift is significant, the rise that should peak at 7 AM instead peaks between 3 and 4 AM. The body reads this surge as its wake signal and responds accordingly. You are not waking at 3 AM because something is wrong with you. You are waking because your cortisol clock has been reset to the wrong time.
“Chronic insomniacs demonstrated significantly elevated 24-hour cortisol secretion compared to healthy sleepers, with the largest elevations occurring during the evening hours and the first half of the sleep period — the precise window during which cortisol should be at its nadir.”

The Sleep Stage Cortisol Specifically Destroys
Not all sleep is equally affected. Cortisol's upstream signal — corticotropin-releasing hormone (CRH) — selectively suppresses slow-wave sleep (SWS, also called N3 or deep sleep), the most physically restorative stage. When CRH is administered to sleeping subjects in controlled settings, the result is a consistent reduction in SWS, an increase in lighter stage 1 and stage 2 sleep, and a fragmentation pattern clinically identical to stress-related insomnia.
Slow-wave sleep is the stage where growth hormone is secreted in its largest daily pulse, where the hippocampus consolidates declarative memory, and where the glymphatic system clears metabolic waste from the brain. These processes do not happen during REM or lighter sleep stages. When chronic cortisol suppresses SWS, it is not making sleep lighter in a vague sense. It is eliminating the stage that restores the body and brain at the cellular level.
“CRH administered during sleep significantly reduces slow-wave sleep while increasing stage 1 sleep and wakefulness. These findings indicate that HPA axis hyperactivity directly impairs sleep architecture through hypothalamic CRH signaling, independent of subjective stress experience.”
Slow-wave sleep normally suppresses CRH secretion — this is the body's own brake on HPA activity during the night. Chronic cortisol reduces SWS. Less SWS means less CRH suppression. Which means more CRH. Which means more cortisol. Which means less SWS the following night. The mechanism is self-reinforcing from the first disrupted night and does not require a new stressor to sustain it.
The Loop That Keeps Running After Your Stress Is Gone
This is the part most sleep content skips — and the part that explains why resolving the stressor does not immediately resolve the sleep. Sleep deprivation itself elevates cortisol the following day, through a mechanism entirely separate from the original stress response.
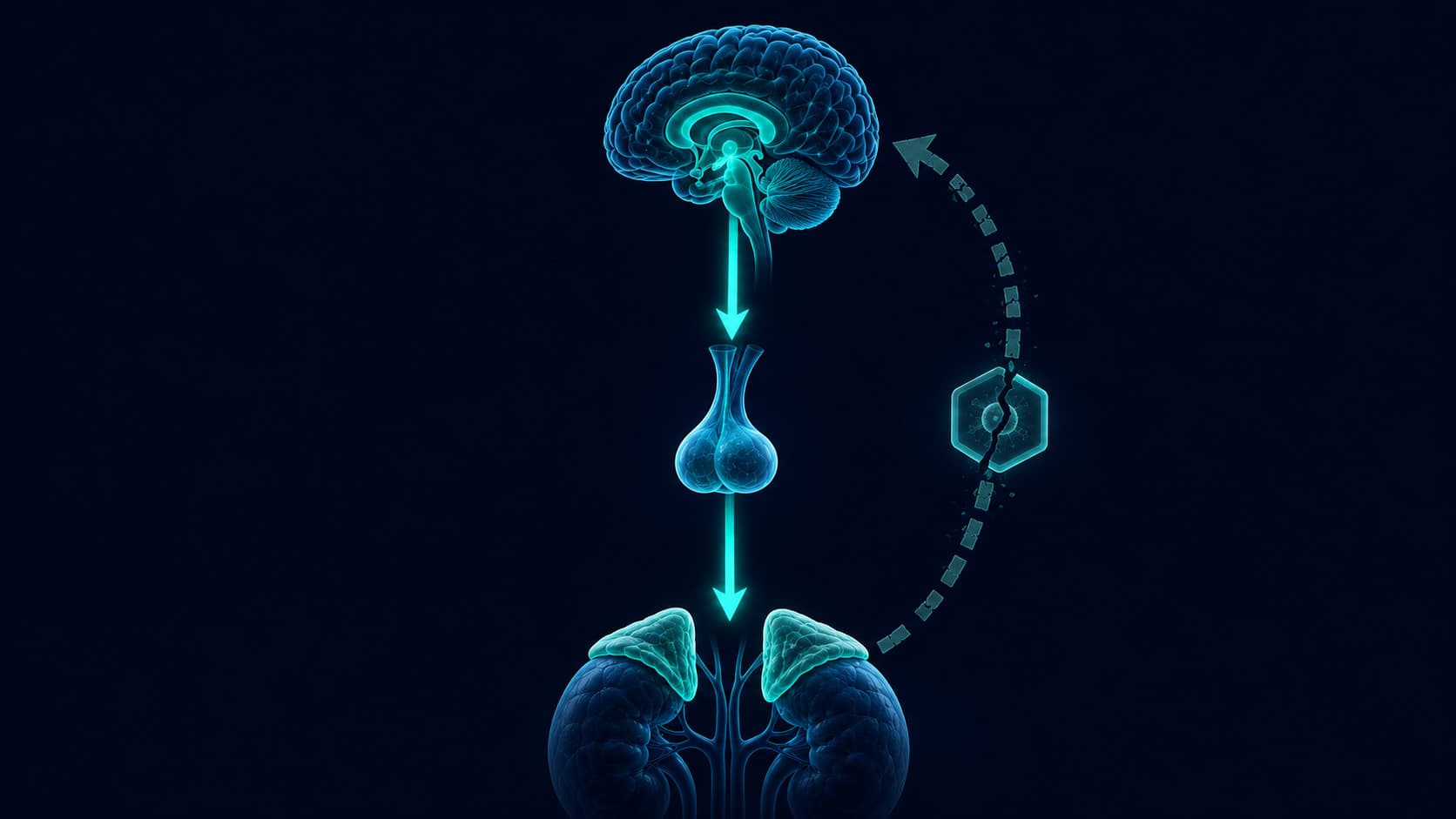
The mechanism: the hippocampus monitors cortisol through glucocorticoid receptors and signals 'enough' when levels are adequate, acting as the body's brake on cortisol production. Sleep deprivation reduces hippocampal glucocorticoid receptor sensitivity — the brake becomes less responsive. Cortisol rises higher the following day and evening. Which disrupts that night's sleep. Which further reduces receptor sensitivity. Which raises the next day's cortisol. The loop runs on the disrupted sleep alone. The stressor is no longer required.
Cortisol fails to reach its nadir — melatonin onset delayed, sleep initiation impaired
CRH-driven suppression of slow-wave sleep — light, fragmented architecture
Premature cortisol surge — body interprets this as wake signal, exits sleep
Sleep deprivation reduces hippocampal glucocorticoid receptor sensitivity — cortisol rises higher
Cortisol enters the evening window already elevated — melatonin suppressed earlier than the night before
Loop tightens with each cycle — original stressor no longer required to sustain it
“One week of sleep restricted to 6 hours per night produced a significant elevation of cortisol levels the following evening — demonstrating that sleep loss alone is sufficient to sustain HPA axis hyperactivation and perpetuate the cycle independently of the original stressor.”

What to Do at 3 AM Right Now
Most sleep content explains why 3 AM waking happens but skips the moment where help is actually needed: you are awake, it is 3 AM, and you need to be functional in four hours. The standard advice — just relax — fails because relaxation is not the mechanism here. Cortisol is. And cortisol has specific behavioral antagonists.
- Do not check your phone. Any lit screen suppresses melatonin re-onset and signals daytime to the suprachiasmatic nucleus. One glance costs 45 to 90 minutes of delayed return to sleep.
- If you have been awake for more than 20 minutes, leave the bed. Staying in bed while awake builds a conditioned association between the bed and wakefulness — the mechanism that turns occasional 3 AM waking into every-night 3 AM waking.
- In a dim room with no overhead light, write down anything active in your mind. Externalizing stops the working memory rehearsal loop that keeps the prefrontal cortex — and the stress response — activated.
- Breathe slowly, not forcefully. A gentle 4-count inhale, 6-count exhale shifts autonomic balance toward parasympathetic dominance, which is the physiological state required for cortisol suppression. Do not strain.
- Return to bed only when you feel sleepy, not after a set time. Sleep pressure is the mechanism — not willpower and not the clock.
The goal at 3 AM is not to fall asleep immediately. It is to prevent the secondary problem: the anxiety about waking becoming the primary driver. When the fear of 3 AM becomes more activating than whatever caused the original cortisol elevation, the sleep disruption outlasts both by months.
What the Research Shows Breaks the Loop
The loop has two effective entry points: the morning light signal and the evening cortisol floor. Neither requires supplements. Both require timing precision and a minimum of six to twelve weeks before the cortisol clock measurably re-anchors.
Morning Light Within 30 Minutes of Waking
Outdoor morning light is the primary calibration signal for the cortisol clock. Natural light exposure within 30 minutes of waking produces a sharper, earlier CAR peak — which means it completes faster, drops lower, and is less likely to spill into the evening window. Ten to fifteen minutes outdoors is sufficient. Overcast sky still works. The mechanism is retinal photoreceptor activation triggering suppression of nocturnal melatonin and a clean cortisol initiation signal that re-anchors the full 24-hour diurnal rhythm.
High impactConsistent Wake Time — Not Bedtime
The cortisol clock is anchored to anticipated wake time, not to when you go to bed. A fixed wake time — held on weekends — is what re-stabilizes the CAR pattern. The body learns when to initiate the morning rise, which prevents the unpredictable early-night surges responsible for 3 AM waking. Varying wake time by more than 45 minutes between weekdays and weekends is enough to delay re-anchoring by days with each cycle.
High impactThe Evening Cortisol Floor
Three inputs directly sustain evening cortisol elevation: bright or blue-spectrum overhead light after 9 PM (signals daytime to the suprachiasmatic nucleus), high-stakes cognitive or emotional processing after 8 PM (activates the HPA axis independently), and caloric restriction in the evening (low blood glucose triggers a compensatory cortisol response). Removing these inputs creates the conditions for the evening cortisol floor to progressively lower over two to four weeks — which is what allows melatonin to rise on schedule.
High impact
The Loop Does Not Break by Sleeping More. It Breaks by Correcting the Signal.
Spending more time in bed — the instinctive response to feeling under-slept — often worsens this pattern. More time in bed with a dysregulated cortisol clock means more time in light sleep, more time in the 3 AM waking window, and more anxiety about lying awake that deepens conditioned arousal. The research on cognitive behavioral therapy for insomnia addresses this directly: sleep compression, not sleep extension, is the clinical intervention for fragmented architecture.
The six-to-twelve week timeline is important for a specific reason: most people expect sleep to improve within days of reducing stress or starting behavioral changes. When it does not, they conclude the approach is not working and abandon it. What is actually happening is that the cortisol clock needs enough consecutive consistent signals to recognize the new pattern and reorganize around it. Not one good night. A pattern the system can measure.
The 3 AM waking that persists after your stress is gone is not evidence that something permanent has happened. It is evidence that a biological loop is still running on data from a period that has ended. The signal that updates that data is not more time in bed. It is a corrected rhythm, applied consistently enough for the system to register the change — and let the old pattern go.
The Cortisol Files continues.
Next: what chronic cortisol does to your immune system — and why you get sick the moment you stop being stressed. In your inbox the week it publishes.
Stay with the seriesGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.