You have had every test done. Your iron is 'in range.' Your doctor said everything looks fine. And you are still exhausted.
Iron and ferritin are not the same thing. Iron is what your body has today. Ferritin is what your body has in storage for the weeks ahead. You can have 'normal' iron and severely depleted ferritin at the same time, and most doctors will not tell you because the standard panel does not check ferritin. The threshold most research uses for fatigue is ferritin under 50 ng/mL. For hair loss, under 40. For restless legs, under 75. Below these numbers, your body is running on empty even when 'today's' iron looks fine. This article explains the exact three tests to ask for, the four numbers that matter, and the alternate-day protocol that raises ferritin faster than the daily iron pill your friend takes.
You have felt this for months, maybe years. You cannot get up in the morning without effort. You need three coffees to function. Your hair is thinner than it was two years ago and you find strands on your pillow. You lose your train of thought mid-sentence. Your legs twitch at night. You have been to your doctor. Your bloodwork came back normal. You have been told to sleep more, meditate more, eat cleaner. And still, you know something is wrong. This article is for the women who have been dismissed. The problem is almost never in your head. It is almost always in what your doctor did not test for.
Iron is what you have today. Ferritin is what you have stored.
Standard iron panels measure serum iron, which is the amount of iron circulating in your blood at the moment of the blood draw. It is a snapshot. It fluctuates by the hour based on what you ate, when you slept, whether you are menstruating, and whether you are recovering from any small inflammation. Serum iron can look completely normal while your body is quietly draining its reserves. Because iron is a snapshot, it tells you almost nothing about whether you have enough iron for the coming weeks.
Ferritin is different. Ferritin is a protein that stores iron in your organs, mainly the liver, spleen, and bone marrow. When your body needs iron for red blood cells, hair follicles, thyroid function, neurotransmitter synthesis, or muscle activity, it draws from ferritin. When ferritin is high, you have runway. When ferritin is low, your body is running on the last of its reserves. And the standard iron panel does not check ferritin unless you ask for it specifically.
Your iron test was normal. Your ferritin was not. No one told you because no one looked.
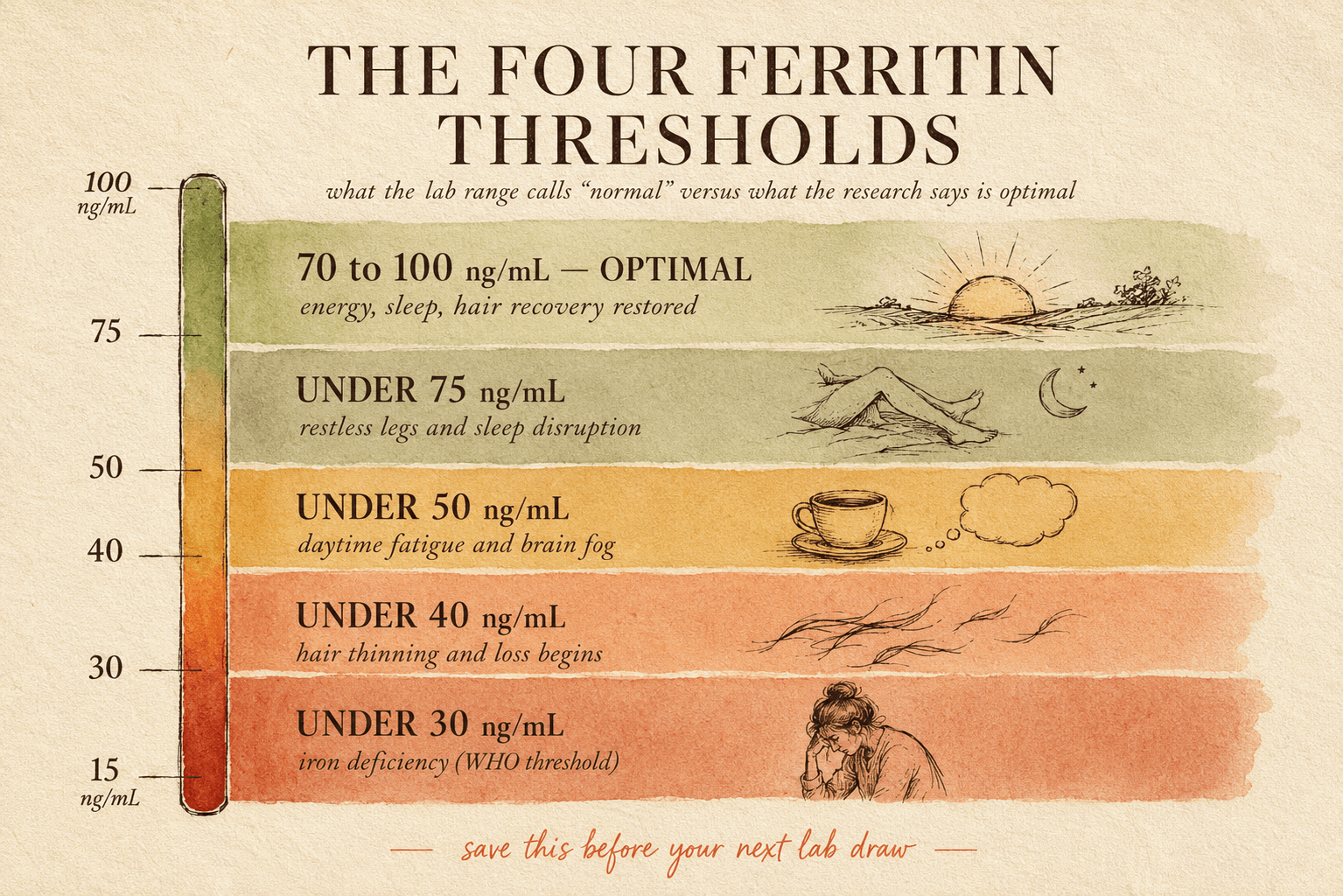
The four ferritin thresholds most doctors do not use
There is 'normal' ferritin, and there is 'optimal' ferritin. Most labs flag ferritin as low only when it drops below 15 or 20 ng/mL, which is when iron-deficiency anemia begins. But your body starts having symptoms long before your ferritin is 'clinically low.' The research on ferritin thresholds for specific symptoms is much stricter than the lab reference range.
Under 75 ng/mL — restless legs and sleep disruption
Multiple studies since 2018 show that ferritin below 75 is associated with restless legs syndrome and fragmented sleep, even in people whose iron looks normal. If your legs twitch at night, if you kick during sleep, if you wake feeling unrested no matter the hours, ferritin is the first place to look.
Under 50 ng/mL — daytime fatigue
This is the threshold that has emerged consistently in the fatigue research over the last decade. Below 50 ng/mL, women report significant fatigue, low energy on effort, exercise intolerance, and cognitive slowness at rates far above baseline. Above 70 to 100, symptoms typically resolve. Between 50 and 70 is the gray zone: many people still feel foggy, but the drop is not as dramatic.
Under 40 ng/mL — hair thinning and loss
Hair follicles are among the most metabolically active tissues in the body, and they need iron to sustain the growth phase. Below 40 ng/mL, the growth phase (anagen) shortens and more follicles enter the shedding phase (telogen). The result: gradual diffuse thinning, more shedding in the shower, thinner ponytail. Most dermatology guidelines now recommend ferritin above 50 to 70 for hair regrowth to be possible.
Under 30 ng/mL — clinical iron deficiency
This is where the standard lab reference finally catches on. Below 30, you meet the WHO threshold for iron deficiency. Below 15, you are in anemia territory. But by the time you reach this level, you have been symptomatic for months, often years. The point of the previous three thresholds is that they let you catch and correct the problem before you get here.
The women whose ferritin is almost always low
Certain populations are almost guaranteed to have depleted ferritin, and their doctors rarely check unless specifically asked. Recognize yourself in these patterns if you fit any.
Menstruating women, especially with heavy periods
You lose 10 to 30 mg of iron per cycle. Over years, especially with heavier flow, you never fully replenish. Standard iron may still look normal because it recovers between periods, but ferritin drops steadily over time.
Chronic small blood losses that outpace dietary iron intake, particularly on plant-based or low-red-meat diets.
Regular periods are not the reason you are tired. Slowly draining ferritin from years of periods without adequate replenishment is.
Postpartum women (within 2 years of birth)
Pregnancy alone drops ferritin by 30 to 50 percent. Blood loss during birth accelerates it. Breastfeeding continues the drain. Most women never fully recover ferritin until 18 to 24 months postpartum, and many never recover at all.
The demands of pregnancy, delivery, and lactation deplete iron stores faster than typical Western diets replace them. Standard postpartum bloodwork rarely tests ferritin.
'Postpartum fatigue' is often ferritin depletion, not just sleep deprivation. Sleep deprivation makes it worse. Fixing ferritin fixes the baseline.
Perimenopausal women (roughly 40 to 55)
Cycles become heavier and more erratic in perimenopause. You may bleed for longer, or twice per cycle, or with clots. This is exactly the phase when ferritin depletes fastest, and exactly when you may also be told 'it is your hormones.'
Perimenopause heavy bleeding drops ferritin quickly, but the symptoms (fatigue, hair loss, brain fog) get attributed to estrogen and progesterone shifts alone. Both are happening. Only one is being addressed.
Perimenopause hormone shifts are real. So is perimenopause ferritin depletion. Check both. Correcting ferritin often removes 40 to 60 percent of the fatigue that gets called hormonal.
Vegetarian, vegan, or low-meat eaters
Plant iron (non-heme) absorbs at 5 to 15 percent efficiency compared to 20 to 30 percent for animal iron (heme). Without deliberate strategy, plant-based eaters trend low ferritin even when their diet looks 'balanced.'
Non-heme iron requires vitamin C in the same meal, avoidance of tannins (tea, coffee) around meals, and often supplementation to reach adequate ferritin.
You do not have to add meat. You have to add strategy: vitamin C at every iron-containing meal, coffee separated from meals by 90 minutes, and periodic supplementation when ferritin drops.
The exact three tests to ask your doctor for
Your standard iron panel checks serum iron and total iron-binding capacity. It usually calculates transferrin saturation. It rarely includes ferritin. The three tests below are the complete picture. Ask for them by name at your next appointment.
- Ferritin (serum ferritin). This is the storage number. This is the one that matters most. Reference range depends on the lab (typically 15 to 200 ng/mL), but optimal is 70 to 100 ng/mL for most women.
- Complete blood count with hemoglobin and hematocrit. This tells you whether iron deficiency has progressed to anemia. You can have low ferritin with normal hemoglobin, and that is the situation you want to catch.
- Iron saturation (transferrin saturation). This measures the percentage of your iron-carrying protein that is currently loaded with iron. Below 20 percent suggests deficiency even when ferritin is borderline.
If your doctor pushes back and says 'we do not usually check ferritin unless there is anemia,' ask them to add it based on your symptoms. Most will agree if you ask specifically. If they will not, direct-to-consumer lab tests (Empower, Rupa, LetsGetChecked in the US, Medichecks or Thriva in the UK) let you order ferritin yourself for under 50 dollars.
How to raise ferritin (and why alternate-day works better than daily)
The old advice was: take iron every day, forever. New research shows this is inefficient. Daily iron doses raise a hormone called hepcidin, which is your body's iron-absorption regulator. When hepcidin is high, your gut absorbs less of the next iron dose. Take iron every day and by day 3, your absorption is cut by half or more.
The 2017 Stoffel study in The Lancet Haematology changed the field. Alternate-day dosing (every other day, not daily) let hepcidin drop between doses, allowing 30 to 40 percent more iron to be absorbed per dose. Same total iron per week, meaningfully more actual absorption. This is the protocol now recommended by many hematology clinics.
The alternate-day ferritin protocol
- 1Day 1
Take iron supplement (usually 40 to 80 mg elemental iron: ferrous sulfate, ferrous bisglycinate, or gentle-iron form) with a source of vitamin C (100 to 200 mg from food or supplement). Coffee, tea, dairy, and calcium at least 90 minutes away.
- 2Day 2
No iron supplement. Eat iron-rich foods with vitamin C throughout the day. Red meat if you eat it, dark leafy greens with lemon, lentils with bell pepper, dark chocolate. Continue avoiding coffee within 90 minutes of iron-containing meals.
- 3Every 8 weeks
Recheck ferritin. Most protocols aim for 70 to 100 ng/mL as the maintenance target. Once you hit target, you can taper to 2 to 3 times per week, then to food-based maintenance.
The reason to check ferritin every 8 weeks and not sooner: iron incorporation into ferritin storage takes 6 to 8 weeks. Test at 4 weeks and you may see very little change even though the protocol is working. Test at 8 weeks and you will see the real trajectory.
The food strategy that actually raises ferritin
Supplements are one lever. Food is the other. The rules for food iron are simple but often broken in typical Western eating patterns.
| Food | Iron per serving | Absorption note |
|---|---|---|
| Beef liver, 100 g | 6.5 mg heme iron | Highest bioavailable iron. Even once per week meaningfully raises ferritin. |
| Red meat (beef, lamb), 150 g | 3-4 mg heme iron | Best combined with dark leafy greens for total meal iron. |
| Sardines or oysters, 100 g | 3 mg heme iron | Convenient for non-red-meat eaters. |
| Lentils, 200 g cooked | 6 mg non-heme iron | Absorption is 5-15 percent. Add vitamin C source (lemon, bell pepper) to same meal. |
| Spinach (cooked), 100 g | 3.5 mg non-heme iron | Cook, do not eat raw. Cooking reduces oxalates that block iron. |
| Pumpkin seeds, 30 g | 2.5 mg non-heme iron | Snack or salad topping. Add citrus dressing for absorption. |
| Dark chocolate 85 percent, 30 g | 3 mg non-heme iron | Convenient. Enjoy after dinner, not with coffee. |
| Blackstrap molasses, 1 tbsp | 3.5 mg non-heme iron | Add to smoothies or oatmeal with vitamin C source. |
The three ferritin mistakes that keep women stuck at 40
→Related readingWhy you wake up tired after 8 hours of sleepWhat to expect week by week
The ferritin recovery timeline
- Week 2 to 3Expected
Sleep quality often improves first. If restless legs were part of your pattern, twitching may reduce. Fatigue often has not shifted yet — do not judge the protocol here.
- Week 4 to 6Patience
Energy on effort starts to change. Stairs feel less heavy. Afternoon fatigue lifts slightly. Brain fog improves. Ferritin has typically moved 10 to 20 points if the protocol is dialed in.
- Week 8 to 10Patience
Ferritin recheck at week 8. Most people who follow the protocol see 20 to 40 point increase. Fatigue is meaningfully better if starting ferritin was under 40. Hair shedding often continues at this stage — hair recovery is slower.
- Week 12 to 16Visible result
Hair shedding starts to reduce. New growth (short hairs at the hairline) starts appearing. Full hair recovery takes 6 to 12 months from ferritin normalization. Energy is close to baseline for most people.
When iron supplementation is not the answer (or is risky)
This article is editorial synthesis, not medical advice. Individual iron needs vary, and iron supplementation carries real risks when taken without appropriate monitoring, particularly for people with hemochromatosis (which affects 1 in 200 people of Northern European descent and is often undiagnosed). Baseline ferritin above 200 ng/mL should be discussed with a physician before any supplementation begins.
What actually changes when your ferritin passes 70
The women who follow this protocol and reach a ferritin of 70 to 100 describe the same experience. Morning energy returns first. The feeling of needing coffee to function fades within weeks. Afternoon crash disappears. Cognitive fog lifts. Sleep is deeper and shorter. Hair shedding slows and then stops. Cold hands and feet warm up. Legs stop twitching at night. Nothing about you has changed at the personality level. But the body running underneath your personality now has the iron to do its jobs. That is what 'baseline' actually feels like.
Most women who correct low ferritin later say the same sentence: I did not realize how tired I had been for how long. The exhaustion had become their normal. Correcting it revealed how much of what they thought was 'me' was actually iron depletion wearing the mask of personality.
You did not become tired. Your ferritin dropped and no one looked.
One women's physiology deep-dive every week.
Next in this series: the ferritin-thyroid connection, the perimenopause blood panel most doctors do not order, and the exact protocol for hair regrowth once ferritin is corrected.
Join the newsletterGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.