Eight hours in bed. Alarm fires. You feel like someone interrupted surgery mid-procedure. The problem is not how long you slept. It is where in the cycle the alarm landed.
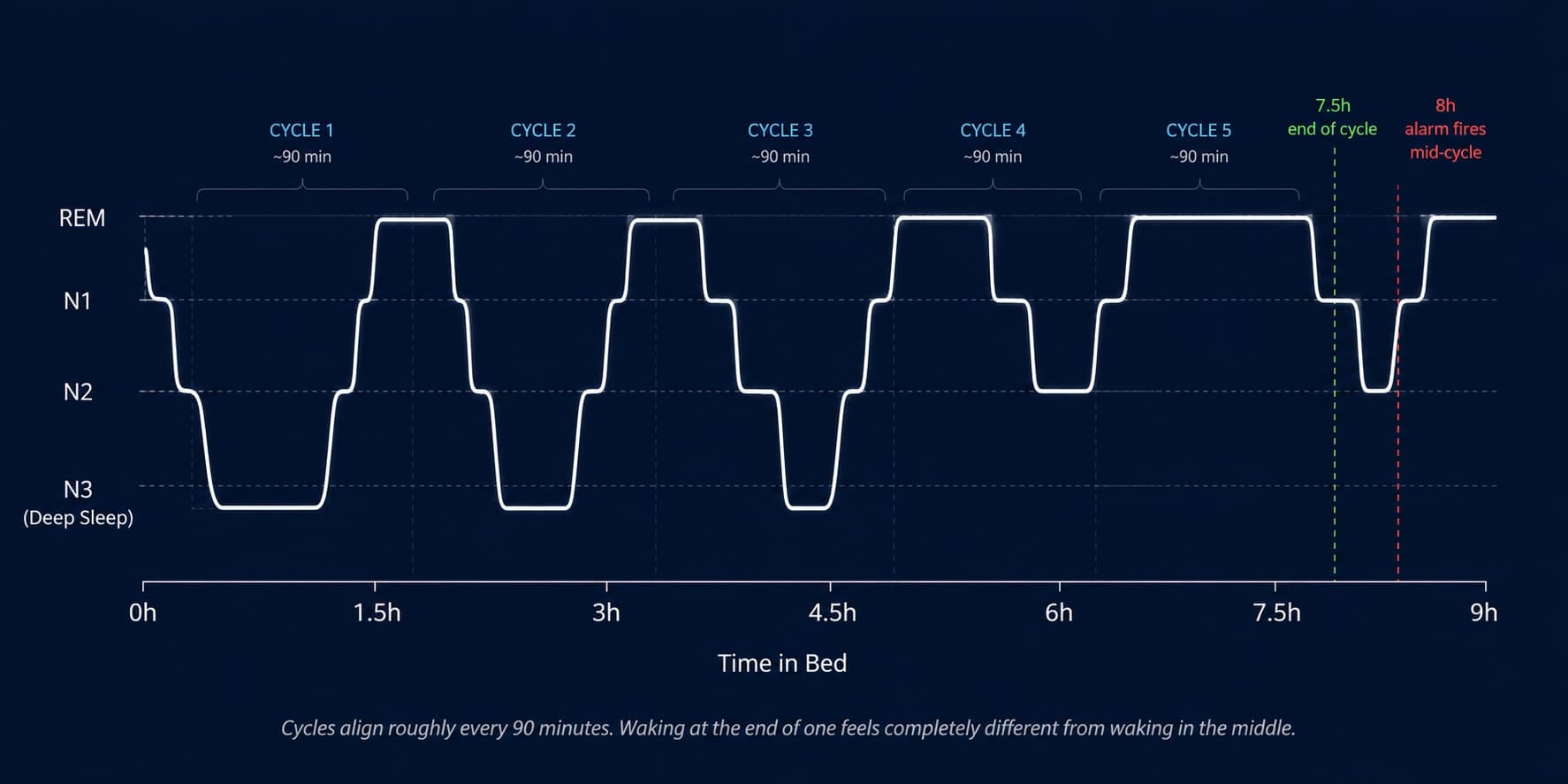
Sleep runs in 90-minute cycles that repeat four to six times a night. If your alarm fires during deep N3 sleep, your brain cannot transition to consciousness smoothly, producing a phenomenon called sleep inertia. In controlled studies, this impairment matches mild alcohol intoxication. Waking after 7.5 or 9 hours (complete cycles) consistently feels better than 8. But the deeper lever is consistency: the same wake time every day stabilizes your circadian rhythm until your body wakes itself before the alarm.
The standard advice is to sleep more. Get eight hours. Maybe nine. But researchers studying non-restorative sleep have found something more specific than duration. It is interruption. Your brain cycles through four distinct stages approximately every 90 minutes, and whether you feel alert or destroyed at 6:47am depends less on total time than on where in that cycle your alarm cuts you off.
This is why some nights of six hours feel restorative and some nights of nine hours leave you exhausted. Duration is a rough proxy. Timing is the actual variable.
The 8-hour myth, in one comparison
What your brain is doing while you are unconscious
Sleep is not a single state. Your brain moves through four stages each cycle: two phases of lighter sleep, one phase of deep slow-wave sleep called N3, and REM, the stage dominated by dreaming. One complete pass takes about 90 minutes. A full night contains four to six of these cycles.
The cycles change as the night progresses. In the first half, N3 deep sleep dominates. This is when the body performs its most critical maintenance: growth hormone release, tissue repair, immune consolidation. In the second half, REM expands and N3 shrinks. The brain shifts from physical repair to emotional processing and memory consolidation.
Cut the night short from either end and you are not just losing hours. You are losing a specific biological function. Miss the first two cycles by going to bed too late and you sacrifice physical recovery. Miss the last two cycles by waking too early and you sacrifice emotional integration. The two halves of the night are not interchangeable.
During deep sleep, a network of fluid channels called the glymphatic system becomes dramatically more active than during wakefulness. Brain cells shrink slightly, widening the spaces between them, and cerebrospinal fluid flows through to carry away metabolic waste including beta-amyloid. This clearance is concentrated in N3 sleep. Fragmenting the night does not just affect how you feel the next morning; it reduces how much biological maintenance actually occurs.
“Sleep is associated with a 60% increase in the interstitial space, resulting in a striking increase in convective exchange of cerebrospinal fluid with interstitial fluid. The restorative function of sleep may be a consequence of the enhanced removal of potentially neurotoxic waste products that accumulate in the awake central nervous system.”
Why the last cycle matters more than the first
Most articles describe sleep cycles as identical loops. They are not. Each successive cycle contains less N3 and more REM. By cycle four or five, deep sleep barely appears. The block that felt like a solid mass in the first two hours has become a thin ribbon by 4am.
This has a practical consequence rarely explained. The reason people who cut sleep short by 60 to 90 minutes feel disproportionately worse is not that they lost N3, which was mostly complete. It is that they lost their final REM block, which was often the longest of the night. REM in the last cycle handles the emotional consolidation your daytime mood depends on. Sacrificing it does not just cost you dream time. It costs you regulation.
This is why a night of 5 hours can leave you physically functional but emotionally raw. Your N3 was largely intact. Your final REM block, the one that would have processed yesterday's stress, never happened.
The last 90 minutes are not the end of your night. They are the part of the night that decides your mood.
Sleep inertia: what actually happens when the alarm fires wrong
When an alarm fires during deep sleep, the brain does not switch on. It transitions slowly, in a specific neurological order. The brainstem activates first: heart rate climbs, breathing shifts. The limbic system comes online next. The prefrontal cortex is last, sometimes lagging 15 to 60 minutes behind the rest of the brain.
That lag has a name. Researchers who study post-waking cognition have documented a reproducible impairment window whose severity varies with the stage of sleep at interruption.
“Sleep inertia is characterized by a period of impaired cognitive performance, reduced vigilance, and subjective sleepiness that occurs immediately upon waking. The severity is influenced by sleep stage at awakening, with awakening from N3 slow-wave sleep typically producing the most severe impairment.”
Controlled laboratory studies have quantified the deficit as comparable to, and in some conditions exceeding, the cognitive effects of mild alcohol intoxication. The confusion you feel when woken mid-cycle is not a subjective impression. It has a measurable neurological signature.
This is why the alarm that lands well feels like confirmation and the alarm that lands wrong feels like violence. In the first case, cortisol has already been climbing for 30 minutes. Your brain was already ascending. In the second case, cortisol is nowhere near its wake-up rise, and the alarm has to force the system awake against a chemical current that is still pointing toward sleep.
The math of 8 hours (and why it usually lands wrong)
Eight hours sounds precise. Clinically, it is arbitrary. If you sleep from 10:30pm to 6:30am, you are targeting approximately the 5.3-cycle mark. The fifth cycle typically ends around the 7h 30min point. The remaining 30 minutes often land you in the early stage of a new cycle, sometimes in N3 again, just as your alarm fires. You slept long enough. You woke at the worst possible moment.
Seven and a half hours (five complete cycles) or nine hours (six complete cycles) consistently feel better. Not because of the total time, but because you are waking at the end of a cycle, when sleep is naturally at its lightest and the brain is already ascending toward wakefulness.
| Alarm at | Bed by (5 cycles, 7h45) | Bed by (6 cycles, 9h15) |
|---|---|---|
| 5:30 AM | 9:45 PM | 8:15 PM |
| 6:00 AM | 10:15 PM | 8:45 PM |
| 6:30 AM | 10:45 PM | 9:15 PM |
| 7:00 AM | 11:15 PM | 9:45 PM |
| 7:30 AM | 11:45 PM | 10:15 PM |
| 8:00 AM | 12:15 AM | 10:45 PM |
8 hours from a random bedtime
- Lands at the 5.3-cycle mark
- Frequently interrupts N3 or early REM
- Sleep inertia likely significant
- Prefrontal cortex impaired 30-60 min
- Feels worse despite the same or more sleep
7.5 or 9 hours (cycle-aligned)
- Exactly 5 or 6 complete cycles
- Alarm fires at natural lightest-sleep point
- Sleep inertia typically minimal
- Often wake seconds before the alarm rings
- Brain is already ascending. Transition is passive.
Your 90 minutes is not everyone's 90 minutes
The 90-minute figure is a population average. Individual cycles run anywhere from 80 to 110 minutes, and the same person's cycles change with age. Children run shorter. Older adults run shorter and lighter, with less N3 and more fragmentation. If your cycle-aligned bedtime consistently misses, your personal cycle length may sit at 85 or 100 minutes rather than 90.
Two weeks of consistent bedtime and wake time reveal your actual number. If you regularly wake spontaneously about 15 minutes before your alarm, your math is correct. If you regularly feel destroyed, adjust bedtime by 15 minutes in either direction and observe.
Why weekend catch-up sleep does not fix Monday
Beyond cycle alignment, timing consistency has an independent effect. Your circadian rhythm is a 24-hour biological clock that regulates alertness, cortisol release, core temperature, and dozens of metabolic processes. When you sleep at 11pm one night and 1am the next, your internal clock does not update cleanly. It receives conflicting signals and cannot build a reliable rhythm.
Researchers call the gap between internal clock time and social schedule social jetlag. A person who sleeps until 10am on weekends but must be up at 7am on weekdays is effectively flying across two time zones every Monday morning. The cognitive and metabolic consequences mirror actual jet lag: impaired glucose metabolism, elevated inflammatory markers, reduced daytime alertness.
In a large European cohort, Roenneberg and colleagues reported that social jetlag was associated with a 33% higher likelihood of being overweight. The mechanism was not caloric. It was circadian misalignment affecting glucose metabolism and appetite hormone timing, independent of total sleep duration.
The reframe worth carrying with you
How many hours did I sleep?
Where in the cycle did my alarm land?
Duration is a rough proxy. Alignment is the actual variable. A cycle-aligned 7.5-hour night beats a mid-cycle 8.5-hour night on every measurable outcome, and the difference shows up within the first two weeks of trying.
The five levers that actually change how you feel in the morning
Anchor your wake time, not your bedtime
Most people try to fix sleep by going to bed earlier. But your circadian clock anchors to your wake time, not your bedtime. Set your alarm at the same time every day, including weekends, for two consecutive weeks. Your body adjusts its sleep pressure drive to match. The wake time is the anchor. Bedtime follows it, not the reverse.
High impactCalculate bedtime backward from your alarm
From your required wake time, subtract 7h 45min (5 cycles plus 15-min sleep onset) or 9h 15min (6 cycles plus buffer). Even a 15-minute shift toward a cycle boundary produces a measurable difference in how you feel. Use the table above.
High impactGive your cortisol awakening response a runway
Cortisol rises 50 to 160% in the 30 minutes after waking, a response that primes alertness. Morning light accelerates it. A pitch-black room followed by a sudden alarm gives your brain no preparation signal. A sunrise alarm that brightens gradually over 20 to 30 minutes, or slightly open curtains, allows the CAR to build before your alarm confirms it. For the full mechanism, see Why You Wake Up Anxious.
High impactThe snooze button makes sleep inertia worse
Each snooze press starts a new sleep cycle your alarm will interrupt nine minutes later, almost guaranteed to land in the lightest stage. Your brain has already registered the start of a new sleep session and suppressed alertness signals. You get the impairment without the restoration. If you need those nine minutes, go to bed 90 minutes earlier. Do not snooze.
Stop alcohol three hours before bed, caffeine eight
Alcohol collapses the first half of your night: it fragments N3 and blocks the deep sleep block your body was building. Caffeine has a five to seven hour half-life; a 3pm coffee is still active at 10pm. Both interventions look small in isolation and matter enormously in combination. The night after a glass of wine at 10pm and a coffee at 4pm is architecturally a different night from the same duration without them.
Critical- Sleeping longer on weekends does not compensate. It creates social jetlag that costs Monday and Tuesday.
- Sleep tracking apps that promise to wake you at 'the right cycle' guess based on movement, not brain state. They are unreliable for stage detection.
- Blue light blockers help at the margins. The mechanism they address is downstream of timing consistency.
- Meditation apps calm arousal but do not reset a circadian clock that is misaligned by two hours.
- 'Just be tired enough to fall asleep' fails because your bedtime problem is usually a cortisol problem, not a fatigue problem.
The first five minutes after your alarm
Even a well-timed alarm can be sabotaged by the first five minutes. Sleep inertia responds to specific inputs. This is the shortest protocol with the largest same-day impact.
The 5-minute post-alarm protocol
5 min- 1Do not close your eyes again. Even 90 seconds re-entering a sleep cycle is enough to deepen inertia.
- 2Sit up within 30 seconds. The postural change signals the autonomic system.
- 3Feet on the floor within 60 seconds. Ground contact activates proprioceptive alertness.
- 4Water before phone. Even 200ml rehydrates blood volume dropped overnight.
- 5Light exposure within 5 minutes. Open the curtains or step to a window. If it is still dark, use a bright indoor light.
- 6Movement within 5 minutes. A short walk to the kitchen counts. Motion resolves inertia faster than any beverage.
When timing does not explain it
For most people, cycle alignment and consistency explain most of the morning fatigue equation. For some, they do not. If you have run this protocol strictly for four weeks and still wake exhausted, the mechanism is likely not architectural. It is medical, and each candidate is straightforwardly diagnosable.
The two-week protocol
What to expect week by week
- Day 1 to 3Expected
Choose the earliest time you regularly need to be up. Set it as your fixed alarm, including weekends. From that wake time, calculate 7h 45min and 9h 15min backward. Start with the shorter target.
- Day 4 to 7Expected
Build a 30-minute wind-down: dim all lights, stop screens, drop room temperature. You are not forcing sleep. You are removing the signals that keep the brain in alertness mode.
- Day 8 to 14Patience
Rate morning alertness 1 to 10 within 5 minutes of waking. Compare weekday to weekend scores. A gap of more than 2 points suggests social jetlag is still interfering.
- After week 2Visible result
Most people begin waking spontaneously 5 to 15 minutes before their alarm. If you do not, adjust bedtime by 15 minutes in either direction. Your personal cycle may run slightly shorter or longer than 90 minutes.
You did not need more sleep. You needed to wake up on the right minute.

Sleep smarter, not just longer
Weekly science-backed insights on sleep, nutrition, and recovery. Straight to your inbox.
Join the newsletterGetClariSync Sleep Desk
Editorial Research · Sleep Science
The GetClariSync Sleep Desk reviews peer-reviewed research in sleep science, chronobiology, and circadian medicine. We focus on journals indexed in PubMed — including Sleep, Sleep Medicine Reviews, Nature Communications, the Journal of Sleep Research, and the Journal of Clinical Sleep Medicine. Each article cites its primary sources, distinguishes correlational findings from causal evidence, and is reviewed for accuracy before publication. We update articles when stronger evidence emerges and post a correction note when we change a substantive claim. We are editorial researchers, not clinicians — for medical concerns, sleep disorders, or persistent insomnia please consult a board-certified sleep physician or your primary care provider.