The wellness industry built a billion-dollar market on one idea: cortisol is the enemy. Lower it, block it, hack it. Here is what that advice systematically leaves out.
Cortisol is a glucocorticoid hormone released by the adrenal glands in response to stress and in a predictable daily rhythm. In the short term, it sharpens focus, mobilizes energy, and maintains blood pressure stability. Chronic exposure to elevated cortisol is what disrupts immunity, metabolism, memory, and sleep. The distinction between a healthy morning spike and a flattened chronic pattern is where the real science lives.
Take cortisol away entirely and you would not feel calm. You would be unable to stand up. People with Addison's disease, a condition where the adrenal glands fail to produce cortisol, experience profound fatigue, dangerously low blood pressure, and an inability to respond to any physical or psychological demand. Without cortisol, a mild infection can become life-threatening. This is not a minor detail. It is the central fact that most cortisol content ignores completely.
The narrative around cortisol follows a familiar wellness arc: stress is bad, cortisol is the mechanism of stress, therefore cortisol is bad. That logic collapses quickly when you look at what the hormone actually does in a healthy body. The problem is not the hormone. It is the pattern.
What Cortisol Is Actually For
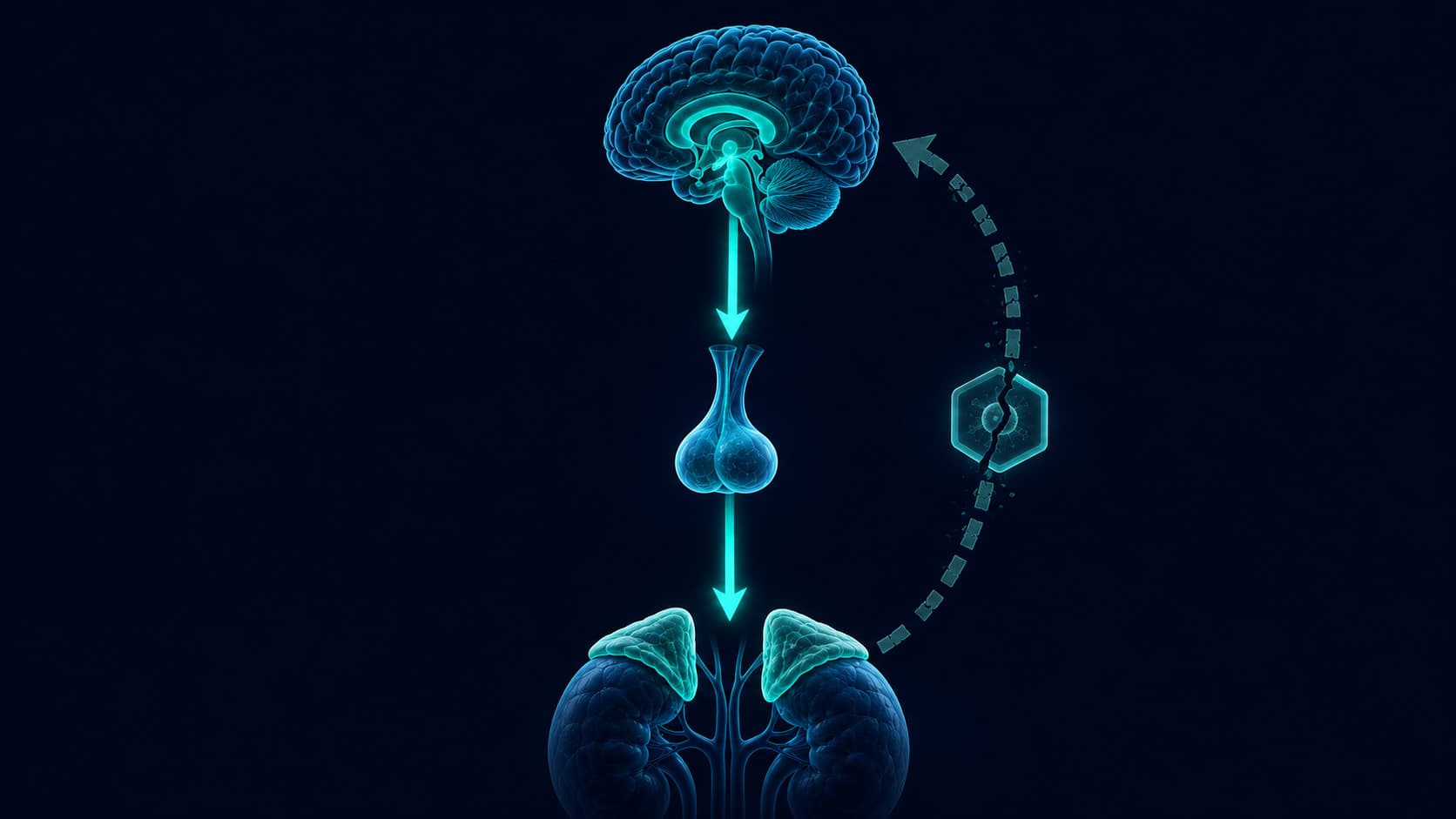
Cortisol belongs to the glucocorticoid family, steroid hormones synthesized from cholesterol in the adrenal cortex. Its release follows the hypothalamic-pituitary-adrenal (HPA) axis: the hypothalamus signals the pituitary, the pituitary signals the adrenal glands, and cortisol enters the bloodstream. That cascade takes roughly 15 minutes from trigger to full effect.
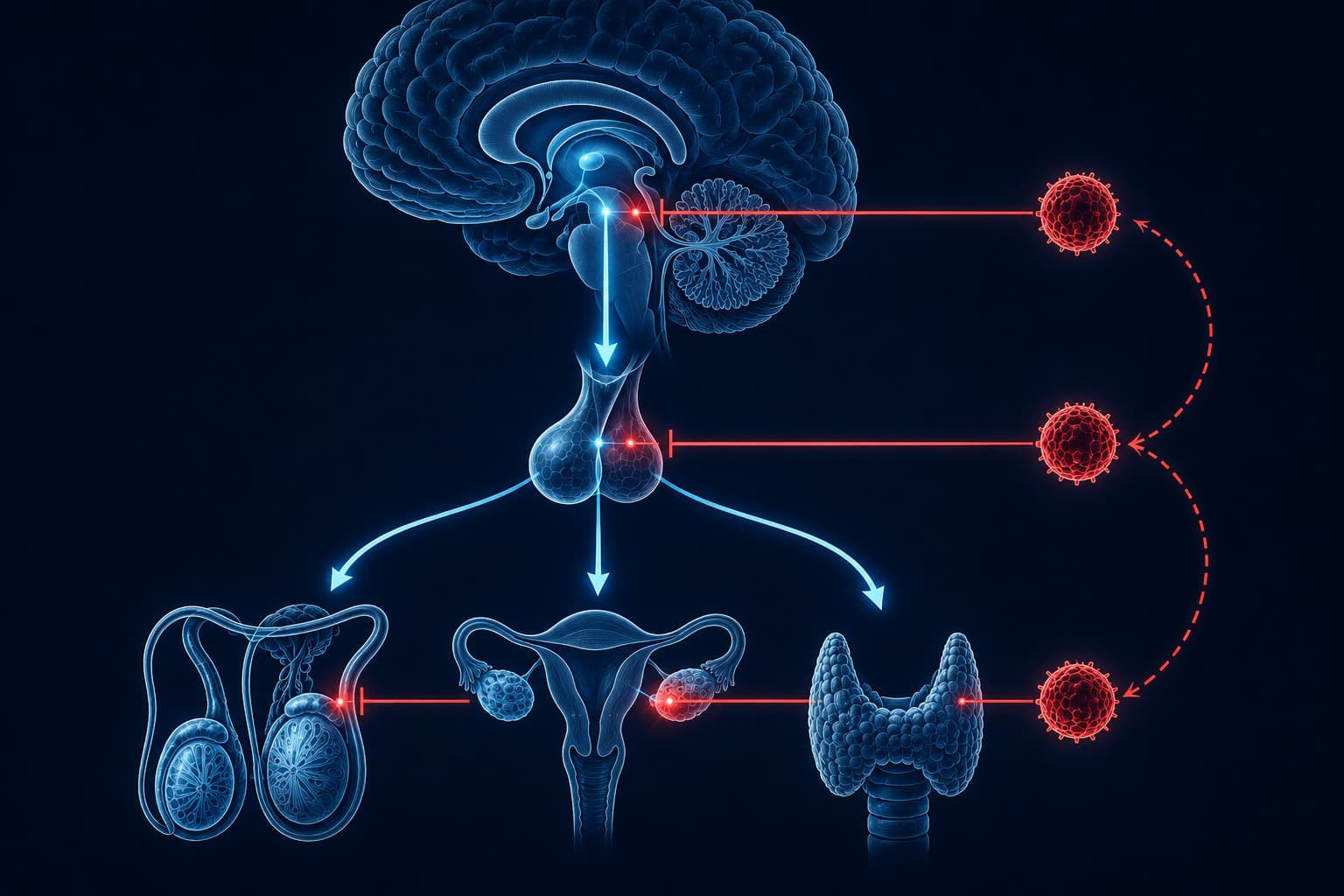
What it does once it arrives is more nuanced than "stress response." Cortisol mobilizes glucose from the liver for immediate energy. It sharpens attention and working memory. It suppresses non-urgent processes, including digestion, reproduction, and immune surveillance, to redirect resources toward the immediate demand. It keeps vascular tone stable so the cardiovascular system can sustain effort. None of that is pathological. That is exactly what a well-designed system is supposed to do.
A landmark review by Sapolsky, Romero, and Munck identified four distinct modes of glucocorticoid action: permissive (enabling other hormones to function), suppressive (dampening inflammation after acute stress), stimulatory (directly activating physiological systems), and preparative (priming the body for anticipated demands). The stress response is not a single mechanism. It is a coordinated multi-mode system where cortisol acts as conductor.
“Glucocorticoids play a critical role in modulating the stress response not by triggering it, but by preparing the organism for the metabolic and physiological demands that stress will impose.”
The Morning Spike: The Most Misunderstood Moment in Your Biology
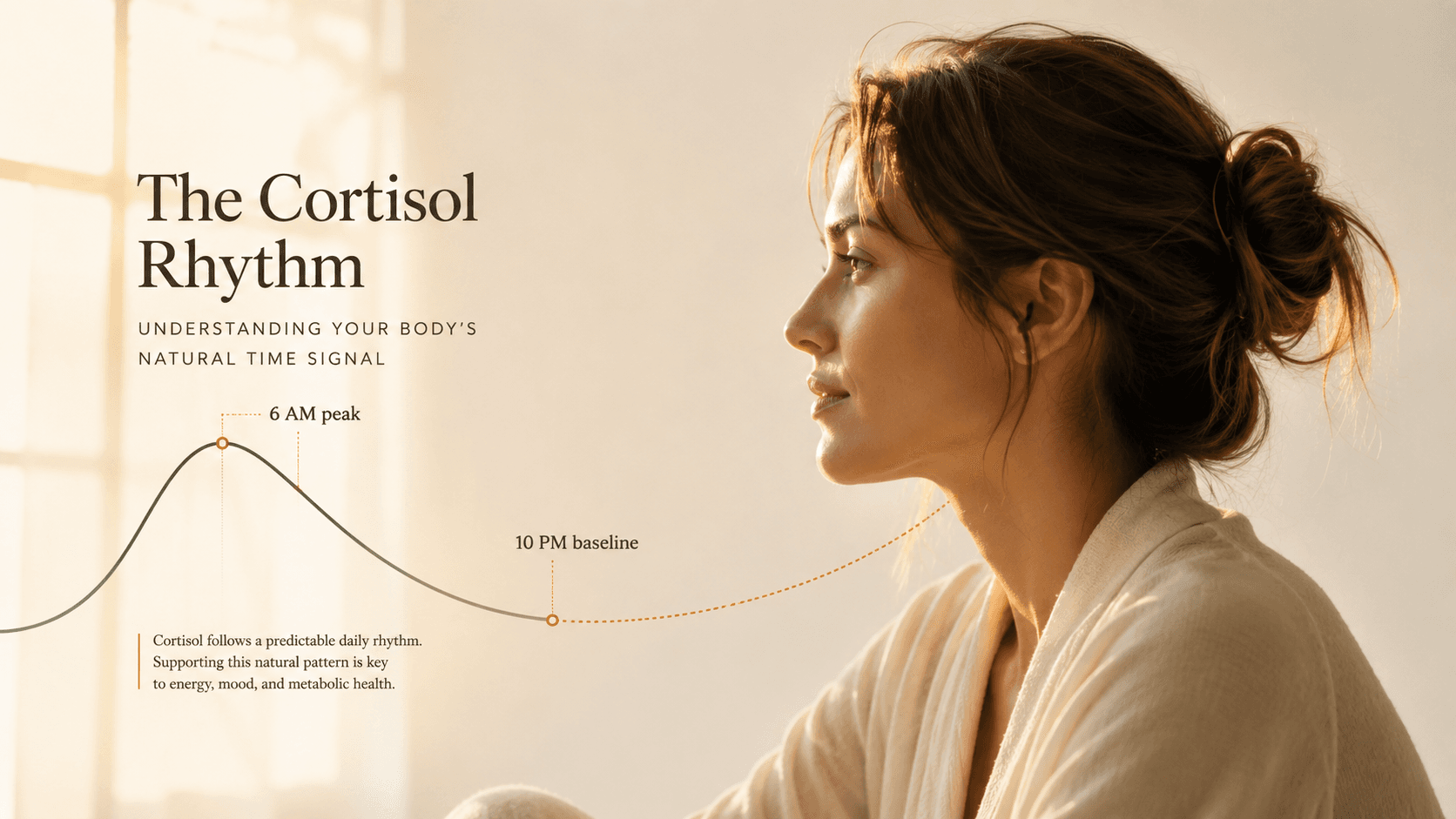
Within 30 to 45 minutes of waking, cortisol levels surge by 50 to 160 percent above baseline. This is not a malfunction. It is called the Cortisol Awakening Response, and it is one of the most important windows in your physiology.
The CAR primes the immune system, activates the prefrontal cortex for executive function, and loads the hippocampus with the working memory capacity needed for the next several hours. Athletes, surgeons, air traffic controllers — anyone operating at high cognitive or physical demand benefits from a robust CAR. Research using the CAR as a biomarker has linked a blunted response to burnout, depression, and chronic fatigue. The morning spike is not the problem. A flat or absent morning spike is.
Fries and colleagues reviewed the Cortisol Awakening Response across occupational and clinical populations. A robust CAR correlated with healthy HPA axis reactivity and cognitive readiness. A blunted or absent CAR was consistently associated with burnout, clinical depression, chronic stress, and PTSD. The CAR captures the health of the entire HPA axis in a single 45-minute window after waking, making it one of the most clinically informative measures in psychoneuroendocrinology.
“The CAR is considered a reliable marker of HPA axis function and is sensitive to chronic stress exposure, burnout, and depressive episodes, suggesting it captures prolonged dysregulation rather than acute fluctuations.”

When the System Turns: Acute vs. Chronic
The line between helpful and harmful is not drawn at high or low. It is drawn at pattern. A cortisol spike during a difficult presentation, a near-accident, a deadline: these are normal activations of a system doing its job. The body handles these well. What it cannot sustain is cortisol that never fully drops.
Chronic psychological stress does something specific: it flattens the diurnal cortisol rhythm. The morning peak becomes blunted. The evening low creeps upward. The gap narrows. Tissues designed to receive cortisol in pulses start receiving it as a continuous signal. That is where pathology begins.
Acute Cortisol (Healthy)
- Sharp spike in response to a specific demand
- Returns to baseline within 60 to 90 minutes
- Sharpens memory, focus, and immune readiness
- Strong morning CAR provides cognitive fuel for the day
- Supports cardiovascular and metabolic function
Chronic Cortisol (Dysregulated)
- Elevated baseline that never fully drops
- Blunted morning CAR, elevated late-evening levels
- Progressive hippocampal volume loss over weeks
- Visceral fat accumulation in the abdominal region
- Immune suppression and increased infection risk
Four Systems Cortisol Damages When It Stays Too Long
Chronic cortisol elevation does not damage one target. It damages several simultaneously, which is why people experiencing chronic stress develop clusters of problems rather than single complaints.
Memory and the Hippocampus
The hippocampus has one of the highest densities of glucocorticoid receptors in the brain. A short burst of cortisol strengthens memory consolidation. Sustained elevation does the opposite: dendritic atrophy and, in prolonged cases, measurable volume loss. Research in populations with major depressive disorder, PTSD, and Cushing's syndrome has consistently documented smaller hippocampal volumes than matched controls.
High impactImmune Surveillance
Cortisol's suppressive effect on the immune system is adaptive in short bursts — it prevents the immune response from overshooting during acute stress. In chronic elevation, that same suppression becomes a liability. Natural killer cell activity decreases. Wound healing slows. Inflammatory cytokines paradoxically increase as the immune system loses sensitivity to cortisol's suppressive signal.
High impactVisceral Fat Accumulation
Abdominal fat cells have significantly higher glucocorticoid receptor density than subcutaneous fat. When cortisol is chronically elevated, it preferentially drives fat storage into the visceral compartment — the metabolically active fat surrounding the organs. This type of fat carries greater cardiovascular and metabolic risk than fat stored elsewhere. The mechanism is direct: cortisol activates lipoprotein lipase specifically in visceral adipose tissue.
High impactSleep Architecture
Cortisol and melatonin operate on opposing rhythms. As cortisol rises in the morning, melatonin falls. As melatonin rises in the evening, cortisol should be low. Chronically elevated evening cortisol delays melatonin onset, suppresses slow-wave sleep, and increases nighttime awakenings. The result is a compounding loop: poor sleep further elevates next-day cortisol reactivity, which produces poorer sleep the following night.
High impact“Women with greater stress-induced cortisol reactivity showed disproportionate fat distribution in the abdominal region, consistent with glucocorticoid-driven preferential activation of visceral adipose tissue receptors.”
Why Adrenal Fatigue Is Not a Real Diagnosis
Adrenal fatigue is one of the most popular concepts in wellness. It appears in supplement marketing, in functional medicine clinics, in influencer content viewed millions of times. It is not recognized by any major endocrinology body. It has no validated diagnostic criteria. And its core mechanism, that the adrenal glands become exhausted from overuse, is not what the research shows.
- The adrenal glands do not wear out from chronic stress — they are robust organs capable of sustained cortisol production
- Chronic stress does not deplete the glands; it desensitizes the HPA axis receptors that regulate cortisol output
- The fatigue people experience is real — the mechanism is receptor downregulation, not glandular depletion
- Adrenal support supplements have no clinical evidence for efficacy against HPA dysregulation
- Actual adrenal insufficiency (Addison's disease) is a serious medical condition requiring physician diagnosis
What actually happens under chronic stress is more specific. The HPA axis does not produce less cortisol because the glands are tired. It produces a dysregulated pattern because the feedback receptors, particularly the glucocorticoid receptors in the hypothalamus and hippocampus, lose sensitivity. The signal that should tell the system to stop producing cortisol stops working efficiently. The result looks like fatigue, cognitive fog, and disrupted sleep. The cause is receptor desensitization, not glandular exhaustion.
The term 'adrenal fatigue' was coined by James Wilson in 1998, a naturopath, not an endocrinologist. No peer-reviewed study has ever validated the concept as a distinct medical entity. The Endocrine Society's official position: 'Adrenal fatigue is not a real medical condition.'
Tsigos and Chrousos reviewed the full neuroendocrine response to chronic psychological and physiological stress, documenting how sustained HPA activation leads to glucocorticoid receptor resistance, not glandular failure. The downstream effects include impaired feedback inhibition, hypersecretion of CRH, and disrupted cortisol rhythmicity. This is the mechanism behind the symptoms commonly attributed to adrenal fatigue, and it requires a different intervention entirely.
“Chronic activation of the stress response results in glucocorticoid resistance and altered feedback sensitivity at multiple levels of the HPA axis, contributing to the persistence of dysregulation even after the stressor resolves.”

The Pattern, Not the Level
Most cortisol advice focuses on reducing the number. Lower your cortisol. But a single cortisol reading tells you almost nothing about a person's health. What matters is the daily rhythm: a high morning CAR that returns to baseline by early afternoon, with low evening levels and minimal nighttime cortisol. That is the signature of a healthy HPA axis.
Disruption of that rhythm is what predicts outcomes. A person with chronically high afternoon cortisol and a blunted morning response may show average total daily cortisol, while displaying every metabolic and cognitive marker associated with chronic stress. Pattern is what matters. Not the absolute number.
CAR: cortisol surges 50 to 160% above baseline. Primes immune function, prefrontal cortex, and working memory capacity.
Cortisol remains elevated, supporting sustained attention, glucose availability, and vascular tone. The high-performance window.
Gradual decline. Ideally reaches 50 to 60% of peak by early afternoon. Sustained elevation here is the first marker of dysregulation.
Should be near baseline. Rising evening cortisol delays melatonin onset and disrupts slow-wave sleep.
Minimum levels. Allows restorative sleep, tissue repair, and HPA recovery for the next morning's CAR.
What Actually Reshapes the Pattern
There is no supplement that fixes HPA dysregulation. The interventions with the strongest research support are behavioral, and they work through specific mechanisms rather than blanket cortisol suppression.
- Morning light exposure in the first 10 minutes after waking — light-dark entrainment anchors the circadian rhythm, which synchronizes the HPA axis. A sharper, better-timed CAR follows.
- Sleep continuity before 1 AM — the bulk of HPA recovery and glucocorticoid receptor resensitization occurs during slow-wave sleep in the first half of the night.
- Moderate aerobic exercise, not chronic high-intensity training — acute exercise raises cortisol transiently, but regular moderate exercise increases glucocorticoid receptor sensitivity and restores diurnal rhythm.
- Stable blood glucose throughout the day — hypoglycemia is a direct cortisol trigger. Skipping meals, extended fasting without preparation, and large glucose spikes all activate unnecessary HPA output.
What does not work: attempting to suppress every cortisol rise. The goal is rhythm restoration, not blanket suppression. The body requires cortisol to function. The work is in making the pattern clean.
→RelatedWhy You Wake Up Anxious: The Cortisol Awakening Response ExplainedThe Cortisol Series
This is the first article in a seven-part series on cortisol, stress biology, and HPA axis function. The next article examines what the research actually shows about cortisol and weight gain, and why the mechanism is more specific than most accounts suggest.
Subscribe for the full seriesGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.