The most common form of magnesium sold in pharmacies worldwide has a bioavailability of roughly 4%. For every 500mg you take, about 20mg reaches your cells. The rest becomes an expensive laxative.
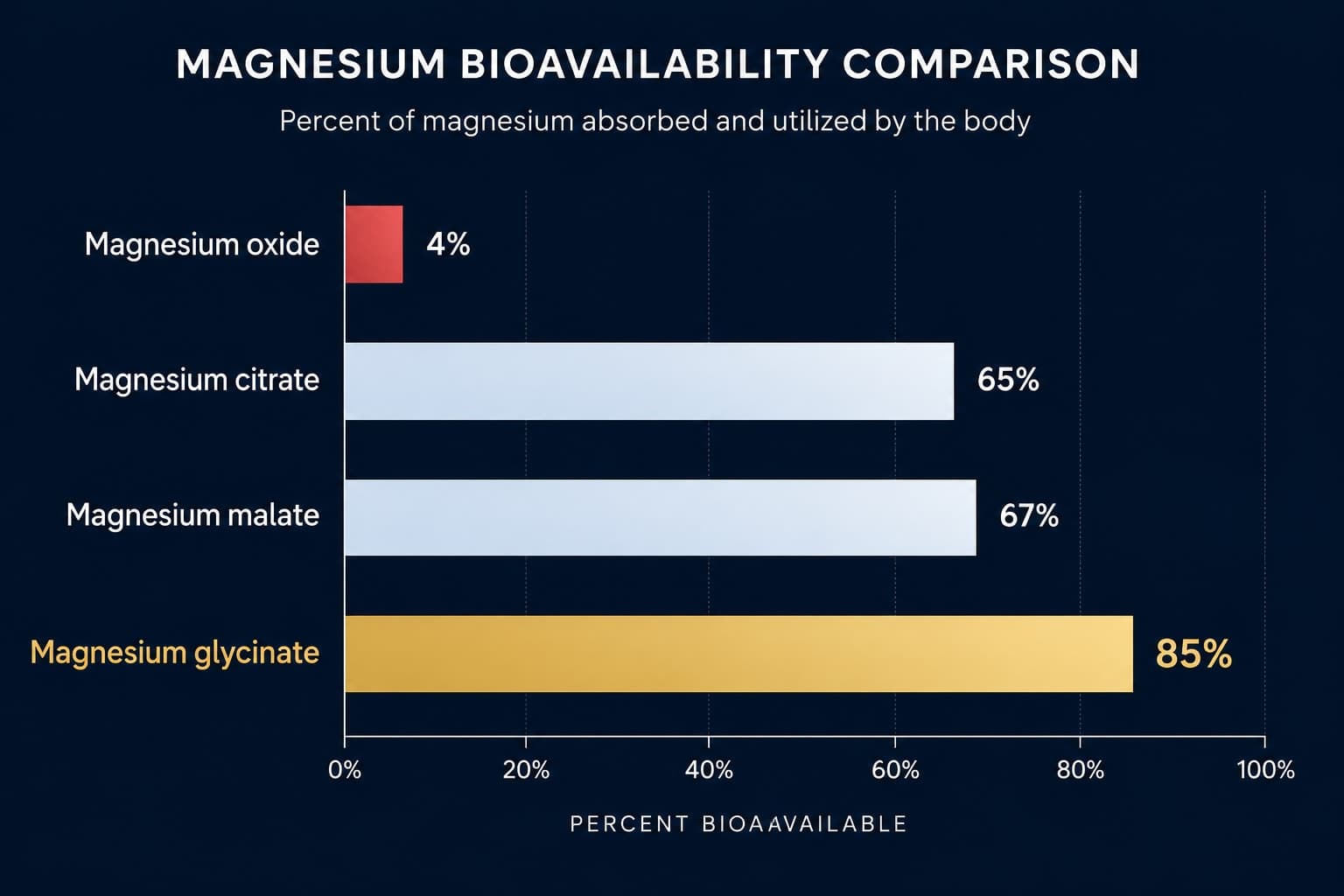
Magnesium is involved in over 300 enzymatic reactions, including GABA synthesis, cortisol regulation, and NMDA receptor blockade, the mechanism that reduces neural excitation. Suboptimal magnesium status affects an estimated 48% of Americans and does not reliably appear on standard blood tests, because serum magnesium reflects less than 1% of total body stores. Form determines almost everything: magnesium oxide absorbs at roughly 4%, while magnesium glycinate reaches 80 to 90% bioavailability. Magnesium glycinate delivers two simultaneous sleep mechanisms: the magnesium itself reduces excitatory neural tone through NMDA blockade, and the glycine component independently improves sleep onset via peripheral vasodilation and core body temperature reduction, a second mechanism documented in its own peer-reviewed trials.
The supplement aisle has several versions of the same mineral. The chelated kind, the citrate kind, the glycinate kind, and the oxide kind near the back for half the price. Most people buy the oxide. Most magnesium research suggests they might as well be buying chalk.
The form problem is not a marketing distinction. It reflects real differences in how each compound behaves in the gut, how much magnesium actually reaches circulation, and in the case of glycinate specifically, whether a second biologically active molecule travels alongside it. Getting this wrong means spending money on a supplement that produces no measurable physiological change.
What magnesium actually does that makes it relevant at 2am
Magnesium is a cofactor in over 300 enzymatic reactions, a number cited constantly without much context. What that number means: magnesium is required for ATP to become biologically active. Every cell that produces energy needs it. Muscle contraction, protein synthesis, DNA repair: all require magnesium. The nervous system effects that matter for sleep and anxiety come through two mechanisms.
First, magnesium is a natural antagonist of NMDA receptors, the glutamate receptors responsible for excitatory signaling. At rest, magnesium sits inside the NMDA channel and physically blocks it. When magnesium levels drop, that block weakens. The result is increased neural excitability: a brain that is harder to quiet, more reactive to stress signals, and more prone to the kind of rumination that turns lying down into an extended monologue about everything that went wrong.
Second, magnesium supports GABAergic function. GABA is the brain's primary inhibitory neurotransmitter, the system benzodiazepines target at much higher intensity. Magnesium does not activate GABA receptors directly, but it supports the synthesis and signaling environment that allows GABA to function effectively. A magnesium-depleted nervous system runs in a chronic low-grade excitatory state. That state does not feel dramatic. It feels like a low-level hum that never quite turns off.
Analysis of NHANES dietary data found approximately 48% of Americans consume less than the estimated average requirement for magnesium. The researchers distinguished clinical hypomagnesemia, which is rare and requires medical intervention, from suboptimal status: insufficient intake to support optimal function without meeting the threshold for clinical deficiency. Suboptimal status does not reliably appear on standard serum magnesium tests, because serum magnesium represents less than 1% of total body magnesium. The kidneys maintain normal serum levels by drawing from bone and tissue reserves even as intracellular stores decline. A normal blood test is reassurance that the kidneys are working, not that tissue status is adequate.
This reframes what a normal test result actually means. The body treats serum magnesium as a priority to regulate, much like blood glucose. It will cannibalize other compartments to keep the serum reading acceptable. By the time serum magnesium drops, tissue depletion has typically been ongoing for some time. Red blood cell magnesium testing provides a somewhat better measure of cellular status, though it remains imperfect.
The absorption gap that makes most supplements ineffective
Bioavailability is how much of a compound actually reaches systemic circulation after ingestion. For magnesium, the differences between forms are not marginal. They are the difference between a supplement that works and one that does not.
Magnesium oxide is roughly 60% elemental magnesium by weight, the highest concentration of any form. This is why it dominates cheap supplements with impressive-looking dose numbers. The problem is absorption. Studies consistently place its bioavailability at 4% or lower. The high elemental percentage is irrelevant when the compound cannot reliably cross the intestinal wall. What magnesium oxide reliably does is draw water into the colon, which is why it functions as a laxative at therapeutic doses and why lower doses often cause loose stools with minimal systemic benefit.
Low bioavailability forms
- Magnesium oxide: ~4% absorbed, mainly laxative
- Magnesium sulfate (Epsom salt): poor oral absorption
- Magnesium carbonate: low absorption, antacid use
- Common in cheap supplements with high-dose labels
High bioavailability forms
- Magnesium glycinate: 80-90% absorbed, glycine effect
- Magnesium citrate: high absorption, mild laxative at dose
- Magnesium malate: well absorbed, useful for fatigue
- Magnesium threonate: crosses blood-brain barrier (animal data)
Magnesium glycinate is magnesium bound to glycine, an amino acid. The chelation dramatically improves intestinal absorption: the compound enters the gut wall via amino acid transport channels rather than relying on the passive diffusion that limits oxide. Independent of absorption, glycine becomes a second biologically active compound once the bond is metabolized. This is the mechanism most content fails to mention.
The glycine discovery: why magnesium glycinate does two things at once
Glycine is a nonessential amino acid and inhibitory neurotransmitter. In the brainstem and spinal cord, it functions as a direct inhibitory signal. In the forebrain, it acts as a co-agonist at NMDA receptors. At doses consistent with magnesium glycinate supplementation, its net effect on sleep onset has been studied independently, without magnesium, and the findings are specific enough to be worth understanding on their own terms.
Glycine has been studied in isolation, without magnesium, to determine whether the amino acid component produces its own measurable sleep effect. The question is relevant because if the two compounds act through separate mechanisms, the combination is not redundant — it is additive. The clearest trial on this used a straightforward design: glycine administered before sleep to subjects already reporting unsatisfactory sleep quality, measured against placebo across multiple nights.
“Glycine ingestion before sleep significantly improved subjective sleep quality, fatigue, and daytime sleepiness, with data suggesting the mechanism involves peripheral vasodilation and reduction of core body temperature, a critical physiological trigger for sleep onset.”
When you take magnesium glycinate, you are taking two compounds with independent sleep mechanisms. Magnesium reduces neural excitation by blocking NMDA receptors. Glycine accelerates sleep onset by triggering the temperature drop the brain uses as a sleep signal. Studies comparing magnesium forms will not find this effect in citrate or threonate trials, because the glycine mechanism is absent.
Research comparing magnesium forms should be read with this in mind. A citrate trial measures one mechanism. A glycinate trial measures two. They are not equivalent comparisons.
Cortisol depletes the mineral that calms the stress response
Chronic stress creates a physiological trap. Cortisol mobilizes magnesium from cells into the bloodstream, where it is excreted through the kidneys. Simultaneously, suboptimal magnesium amplifies the HPA axis stress response: the body releases more cortisol under the same stressor when magnesium reserves are low. Stress depletes magnesium. Low magnesium amplifies stress reactivity. The cycle reinforces itself without a clear external signal that it has begun.
This explains a pattern that anyone who has gone through a prolonged difficult period will recognize: a baseline anxiety that outlasts the original stressor, sleep that does not improve even after the situation resolves, and a sensitivity to smaller triggers that was not present before. Some of that reflects psychological adaptation. Some reflects a nervous system running on depleted reserves. The two are not always easy to distinguish from the inside.
“A systematic review of 18 studies found evidence that magnesium supplementation may have a beneficial effect on subjective anxiety in mildly anxious subjects, with effects most pronounced in populations under chronic stress or with known suboptimal magnesium intake.”
The Boyle review is careful about scope. The evidence is strongest for mildly anxious subjects, not clinical anxiety disorders. Magnesium is not a substitute for treatment of anxiety disorders. What it may address is the physiological substrate that chronic stress quietly depletes, the missing input that keeps a nervous system from returning to baseline after the stressor is gone.
What the sleep trials actually found
The most cited controlled trial on magnesium and insomnia is Abbasi and colleagues' 2012 randomized double-blind study in elderly subjects. The design: 500mg magnesium daily for eight weeks, against placebo. What distinguishes this trial from others is scope. It did not measure only subjective sleep quality. It measured hormonal markers alongside it — a combination that is rarer in supplement research than it should be.
“Magnesium supplementation significantly improved sleep time, sleep efficiency, and early morning awakening, with concurrent increases in melatonin and renin concentrations and significant decreases in serum cortisol concentrations in elderly subjects with insomnia.”
Two caveats apply. The population was elderly, a group with characteristically lower magnesium absorption and higher rates of suboptimal status. Effects in healthy younger adults with adequate dietary magnesium intake may be smaller. Second, 500mg is a relatively high dose; standard glycinate supplements provide 200 to 400mg of elemental magnesium, which falls within the evidence-aligned range.
Magnesium threonate and what the research actually established
Magnesium threonate, sold under the trade name Magtein, is the most expensive form and the most aggressively marketed for cognitive benefits. The underlying research is real and was conducted at MIT. The question is what it established and what it did not.
The MIT research behind threonate started from a specific hypothesis: that raising brain magnesium above its normal ceiling might enhance synaptic plasticity in ways relevant to learning and memory. The challenge was delivery. Most magnesium forms fail to meaningfully elevate cerebrospinal fluid magnesium even when absorbed systemically. Threonate was synthesized as a candidate to cross that barrier.
“Elevation of brain magnesium using magnesium-L-threonate significantly enhanced synaptic plasticity in the hippocampus and prefrontal cortex and improved both short and long-term memory in aged rats, effects not achieved by other magnesium compounds that failed to raise cerebrospinal fluid magnesium levels.”
The honest context: this research was conducted in rats. Human trials are limited and more modest in conclusions. The researchers hold patents on the compound, a conflict of interest worth naming. The claim that threonate uniquely crosses the blood-brain barrier in humans has not been independently replicated to the same standard as the animal data. For sleep, there is no evidence that threonate outperforms glycinate. For cognitive function in people with documented suboptimal status, the mechanistic case is worth watching. As a basis for a premium price, the current human evidence does not fully support the marketing.
Dose, timing, and what to actually do
The protocol questions are where most content either becomes vague or overcautious. The evidence supports more specific guidance.
Form and dose
For sleep and anxiety: magnesium glycinate at 200 to 400mg elemental magnesium is the evidence-aligned choice. For general status correction: magnesium citrate is equally well-absorbed and less expensive, though without the glycine component. Avoid magnesium oxide for any therapeutic purpose. The Institute of Medicine sets the tolerable upper intake level from supplements at 350mg per day; above this, gastrointestinal effects become more likely in some individuals.
High impactTiming
For sleep: 30 to 60 minutes before bed. Glycine's peripheral vasodilation and temperature-reduction effects begin within 30 to 45 minutes of ingestion. Taking magnesium with a light meal improves absorption and reduces gastrointestinal irritation risk. A full meal is not required.
High impactWhat interferes with absorption
High-dose calcium taken simultaneously competes with magnesium for intestinal absorption; space them by at least two hours if both are used. Zinc above 40mg per day also competes. Vitamin D supports magnesium utilization; chronic vitamin D deficiency reduces the effectiveness of magnesium supplementation. Alcohol and diuretics increase renal magnesium excretion and raise daily requirements.
High impactCalcium and magnesium are physiological antagonists: calcium drives muscle contraction and neural excitation, magnesium drives relaxation and inhibition. Modern diets are high in calcium and low in magnesium. Most traditional diets showed the opposite ratio. The balance between the two, not just the absolute level of either, shapes resting neural tone.

Magnesium is not a sedative. It does not produce sleep. What it does is remove a physiological obstacle: the excess excitatory tone that suboptimal magnesium permits. For people with adequate status, supplementation produces little observable effect. For people with suboptimal status, it removes something that was quietly working against them, which is a different thing from adding something new.
Nutrition science without the supplement industry framing
GetClariSync covers what peer-reviewed research actually shows about nutrition, sleep, and daily performance. No affiliate incentives.
Get the newsletterGetClariSync Nutrition Desk
Editorial Research · Nutritional Science
The GetClariSync Nutrition Desk reviews research in nutritional biochemistry, metabolism, and dietary science. We read across the American Journal of Clinical Nutrition, the British Journal of Nutrition, the Journal of Nutrition, Nutrients, and Cochrane Reviews — and we are explicit about what the evidence shows and where it is weak. We do not promote restrictive diets, supplements, or single-food claims unsupported by replicated research. We are editorial researchers, not registered dietitians or physicians — please consult a qualified nutrition professional or your doctor before significant dietary changes, especially if you have a health condition, take medication, are pregnant, or are managing a chronic disease.