
You used to sleep. Since forty something, three in the morning has become the loudest hour of your day.
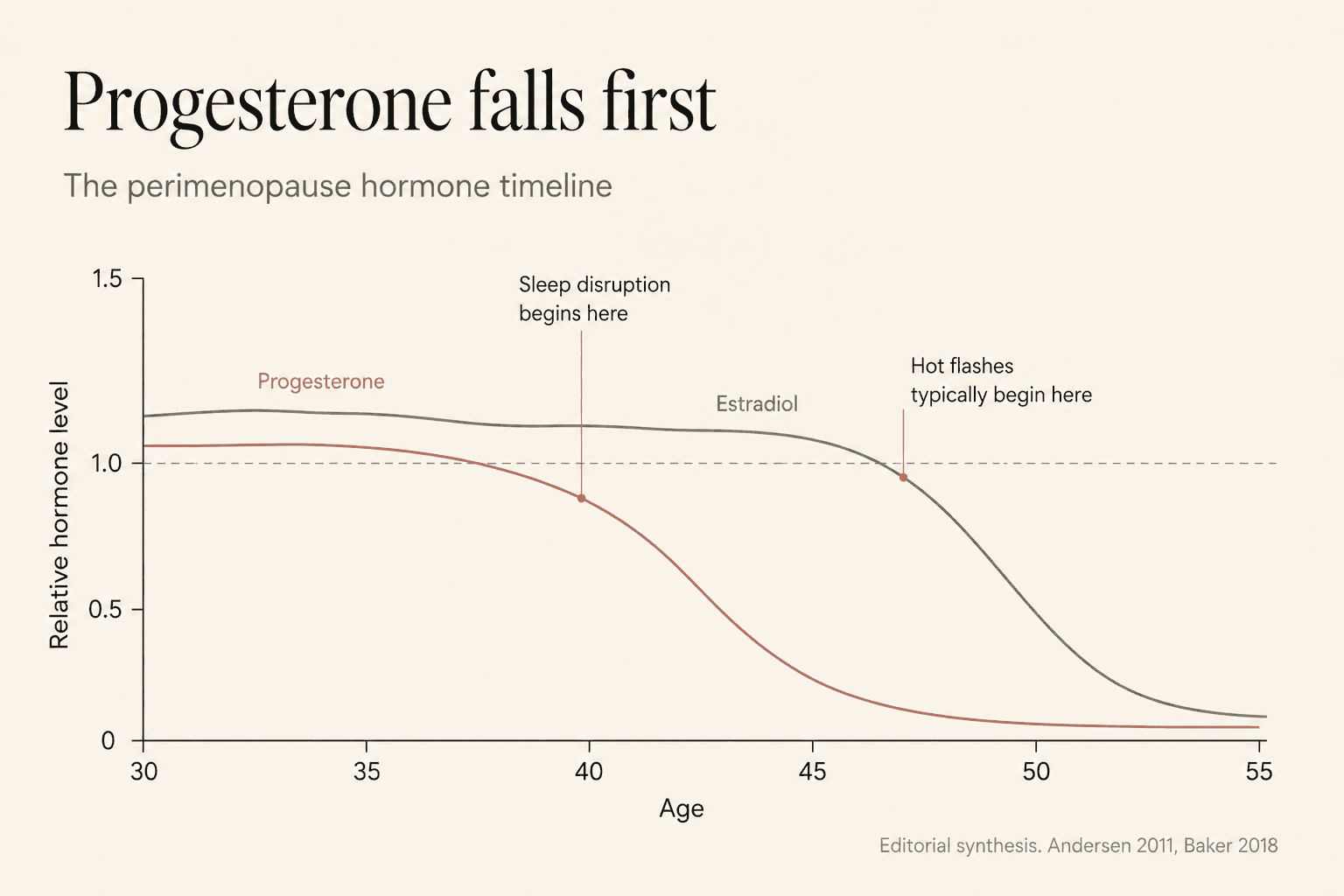
Perimenopause insomnia is not caused by estrogen decline alone. Progesterone falls first, often five to ten years before periods change, and its collapse removes the brain's natural sedative. Estrogen fluctuations then destabilize temperature and REM, and cortisol shifts earlier into the night. The 3am wake-up is the intersection of these three mechanisms, not a personal failure to relax.
The first sign is rarely dramatic. You fall asleep at eleven, exactly the way you always have. Then something wakes you at 3:04. Not a sound. Not a dream. A quiet, precise alertness that arrives in your chest before it reaches your mind. You lie there. You count breaths. You calculate how many hours are left. By 4:30 you give up. By 6:00 the day has already lost.
You mention it to your doctor. She talks about stress. You try magnesium. You try mouth tape. You try a cooler room. Some nights are better. Most nights are not. The internet tells you it is hormonal. The internet tells you it is cortisol. The internet tells you it is trauma. Nothing tells you which, or why now, or what to actually do.
There is a reason. And it is not the reason most articles give you.
Why perimenopause insomnia is not an estrogen problem
The standard explanation blames estrogen. Estrogen drops, sleep breaks. This is not wrong, but it is not what happens first.
Progesterone is the hormone that quiets you. It is metabolized into allopregnanolone, a molecule that binds to the same brain receptors as benzodiazepines. When progesterone is abundant, the brain has a natural sedative circulating through it every night. When progesterone drops, that sedative disappears.
Allopregnanolone, the primary metabolite of progesterone, is one of the most potent positive modulators of the GABA-A receptor known in human biology. When progesterone declines, GABA signaling weakens. When GABA signaling weakens, the sympathetic nervous system loses its brake. The result is not exhaustion that fails to become sleep. It is exhaustion combined with an inability to lower arousal.
The critical detail almost every article omits: progesterone drops before estrogen does. It starts declining in the mid-thirties. By forty, most women are already producing significantly less progesterone during the second half of each cycle. Estrogen may still be within a normal range. Periods may still appear regular. Nothing looks wrong on standard bloodwork.
·2011·Journal of Sleep ResearchBut the sedative that used to arrive each night has thinned. The brain that used to power down at 10:30 now hums. This is why women in their late thirties and early forties start losing sleep years before any doctor calls it perimenopause.
You did not lose the ability to sleep. You lost the hormone that made sleep effortless.
The estrogen chaos that fragments the rest of the night
Estrogen does not decline in perimenopause. It swings. High one week, low the next, high again, then suddenly low for a stretch. The hypothalamus, which uses estrogen to calibrate body temperature, cannot keep up. Its thermostat becomes hyperreactive. A tiny rise in core temperature that would have been ignored at thirty triggers a full sympathetic response at forty five.
This is what a night sweat is. Not a symptom of overheating. A symptom of a temperature control system that has lost its calibration. Every micro-flash pulls you out of REM. You may not remember waking. Your sleep tracker records seven hours. Your body knows you slept in fragments.
Polysomnography studies in perimenopausal women show significant reductions in slow-wave sleep and REM density, and increased arousal frequency, in women who report their sleep as still acceptable. By the time subjective insomnia is reported, the underlying architecture has already been degrading for years.
Estrogen also modulates serotonin, which modulates melatonin. When estrogen swings, melatonin secretion becomes irregular. The signal that used to reliably tell your pineal gland when to release its evening pulse now arrives late, arrives short, or arrives at the wrong intensity.
The nights you feel wired at bedtime are usually estrogen peaks. The nights you fall asleep fast but wake at 2 or 3 are usually estrogen troughs. This is why perimenopause insomnia is unpredictable. It is not one problem. It is a hormone in constant motion, moving through a brain that used to trust it.
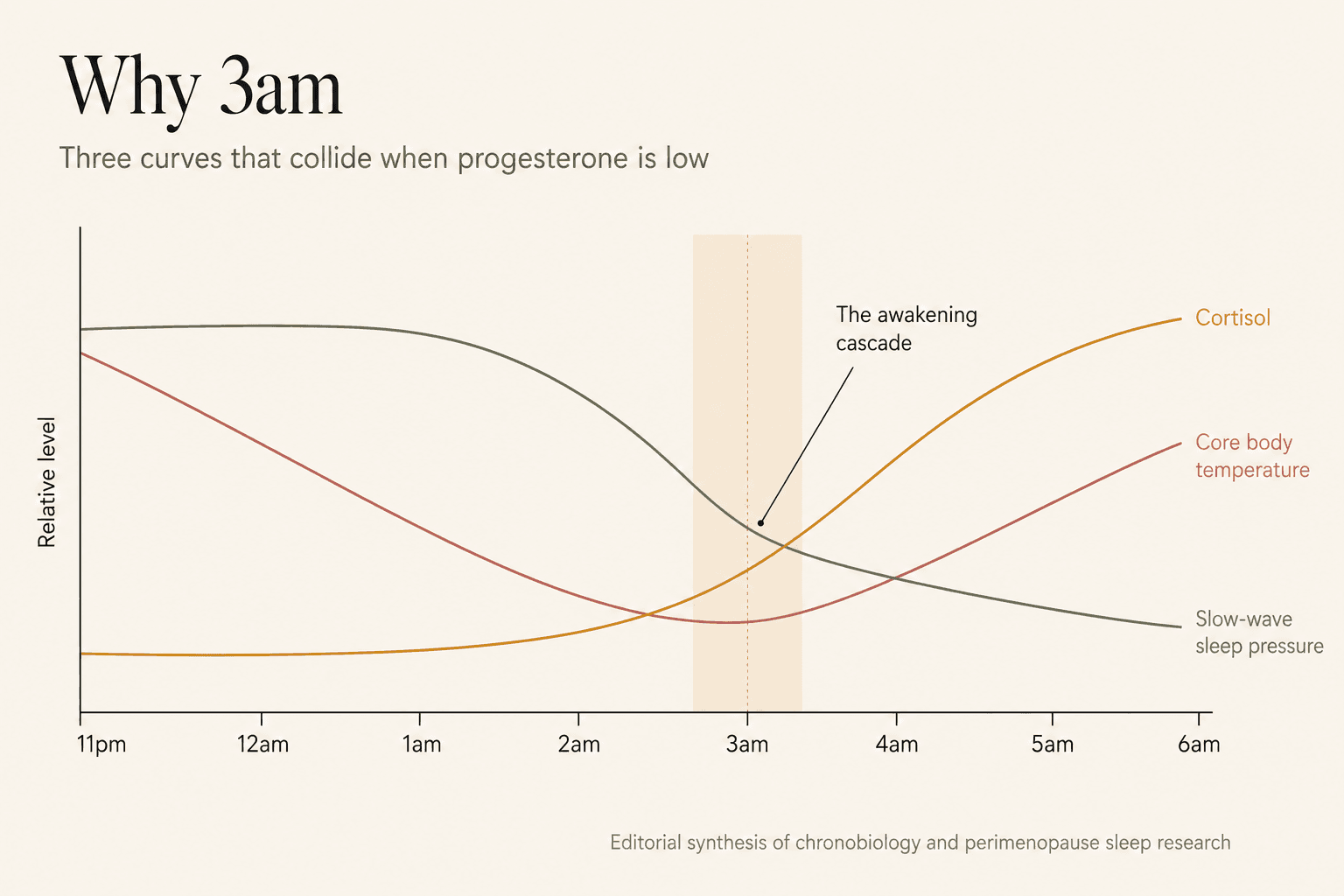
Why 3am specifically
3am is not random. It is the intersection of three curves that used to sit safely apart.
- 1Core body temperature reaches its lowest point Around 3 to 4am, the body normally sits at its deepest thermal minimum. In perimenopause, the damaged thermostat overshoots and triggers a compensatory heat surge. This is what wakes you before you register a hot flash.
- 2Cortisol begins its anticipatory rise The Cortisol Awakening Response does not start at 7am. It begins its climb around 3 to 4am. In perimenopause it climbs earlier and steeper. A brain with no GABA brake cannot ignore this rise.
- 3The first deep sleep block ends The deepest slow-wave sleep concentrates in the first 90 to 120 minutes and the block around 3am. When progesterone is low, this block was already thinner. When it ends, there is no cushion of drowsiness left.
In a woman with normal hormones, these three events happen quietly, in sequence, without waking her. In perimenopause they collide. The alert is not psychological. It is the sum of a nervous system with no brake, a temperature system that overshoots, and a stress axis that fires early.
This is why the 3am wake-up feels different from ordinary insomnia. It is not that you cannot fall asleep. You woke up because your body could no longer stay asleep on its current hormone budget.
What most sleep advice cannot fix in perimenopause
The standard sleep hygiene playbook was written for a nervous system with adequate progesterone. That system responds to blue light reduction, colder rooms, and consistent bedtimes because the underlying sedation machinery is intact. In perimenopause, the machinery is what changed. Adjusting the room does not fix the receptor.
- Melatonin alone rarely holds. The problem is not signaling. It is that GABA cannot suppress arousal once you are woken.
- Cutting caffeine helps at the edges but does not address the missing progesterone effect. Women who never drank caffeine still develop this insomnia.
- Meditation cannot lower arousal that has a receptor-level cause. It can help you tolerate 3am. It does not stop the waking.
- CBT for insomnia works, but slowly, and its assumptions about hyperarousal do not fully match the perimenopause mechanism.
- Blue light reduction is useful but not sufficient. The circadian problem is downstream, not upstream, of the hormone problem.
This does not mean the advice is wrong. It means it was written for a different problem. Perimenopause insomnia responds to a different set of levers.
The four levers that actually hold
None of the following are a cure. They are the levers that, when combined, restore enough sleep architecture to change the trajectory of a perimenopause year. Applied for six to twelve weeks, they typically reduce night wakings by more than half in women who apply them consistently.
Support the GABA pathway with glycine and magnesium
Glycine is a co-agonist at the same receptor system that allopregnanolone modulates. Magnesium glycinate provides both the ion and the amino acid. Taken 45 to 60 minutes before bed at 300 to 400mg of magnesium, it partially compensates for the missing progesterone-mediated GABA support. This is not a placebo effect. It is a receptor workaround.
High impactCool the bedroom to 16 to 18 degrees Celsius
The thermoregulation problem in perimenopause is that the hypothalamus overshoots on tiny temperature rises. A cooler room reduces the frequency and amplitude of these overshoots. This is not comfort optimization. It is a mechanical reduction of the input the broken thermostat overreacts to.
High impactAnchor a morning light dose within thirty minutes of waking
Ten to fifteen minutes of outdoor light between 6:30 and 8:00am advances the cortisol curve and stabilizes melatonin release fifteen hours later. In perimenopause, where the endogenous melatonin signal is weaker, external circadian anchoring becomes more important, not less.
High impactStop eating three hours before sleep
Late glucose signaling forces liver activity to peak between 1am and 3am, which coincides with the fragile deep sleep block. Empty the digestive system by 7pm and the pancreas can rest while the liver detoxifies quietly. This is one of the interventions with the fastest measurable effect on 3am wakings.
Critical
The 3am playbook: what to do when it happens
Waking at 3am becomes worse when the reaction to waking is anxious. The heart rate climbs, cortisol climbs, and the possibility of falling back asleep collapses. The point of a 3am protocol is not to force sleep. It is to prevent the arousal cascade from taking over the next 90 minutes.
The 3am de-escalation protocol
20 min- 1Do not check the time. If you must, glance once, then look away.
- 2Stay horizontal. Sitting up or leaving the bed signals the brain that the night is over.
- 3Slow the exhale. Inhale four seconds, exhale eight seconds. Repeat for at least four minutes. The extended exhale is the vagal brake.
- 4Name where you feel the alertness. Chest? Throat? Behind the eyes? Naming reduces the amygdala response.
- 5If your mind loops on a task, write one sentence on a bedside notebook. This releases the loop without engaging with it.
- 6Accept that you may not fall back asleep. Paradoxically, this releases the pressure that keeps you awake.
This does not always work. On some nights, no protocol will hold. The goal is not perfect nights. The goal is to reduce the number of catastrophic ones.
The hormones your doctor may not have measured
Standard perimenopause testing measures FSH and sometimes estradiol. It rarely measures progesterone at the right point of the cycle. It almost never measures free T3, morning cortisol at 8am, or fasting insulin. Yet each of these can drive night waking independently.
| Test | When to draw | What abnormal suggests |
|---|---|---|
| Progesterone | Day 21 of cycle if still menstruating | Luteal insufficiency, likely GABA support deficit |
| Estradiol | Day 3 and day 21 if possible | Fluctuation amplitude, thermal instability risk |
| Morning cortisol | Between 7 and 9am | HPA dysregulation, likely early awakening |
| Free T3 and TSH | Fasting morning | Thyroid contribution to fragmented sleep |
| Ferritin | Fasting morning | Iron deficiency can worsen restless legs and arousal |
| Fasting insulin | 12 hour fast | Metabolic component of nocturnal waking |
This is not a demand list. It is a conversation starter with a clinician who is willing to look past FSH. Many are not. Finding one who is remains one of the most useful acts of self-advocacy in this transition.
Hormone therapy is not the villain it was told to be
The Women's Health Initiative study, published in 2002, terrified a generation of women away from hormone replacement therapy. Its findings, particularly on older women taking a specific synthetic combination, were extrapolated far beyond what the data supported. Modern reanalysis, and modern formulations, tell a substantially different story.
For many women in early perimenopause with severe sleep disruption, low-dose transdermal estradiol combined with oral micronized progesterone at bedtime addresses both mechanisms this article describes. The estradiol stabilizes temperature and REM. The progesterone restores the allopregnanolone signal and often restores sleep continuity within weeks. This combination is not for everyone. It is genuinely transformative for some.
The best time to have this conversation with a clinician is early, not late. Progesterone in particular is easier to restore before menstrual cycles have fully stopped.
What recovery actually looks like
A realistic timeline with structured intervention
- Week 1 to 2Expected
Nervous system begins to notice consistent bedtime, morning light, and cooler room. Sleep onset improves before continuity does.
- Week 3 to 6Patience
3am wakings begin to space out. Some nights hold. Others do not. This is the frustrating middle phase where consistency matters most.
- Week 6 to 12Visible result
The frequency of catastrophic nights drops significantly. Sleep architecture, measured on a tracker, shows longer deep sleep blocks.
- Month 4 to 12Visible result
For women who add hormone therapy or a targeted supplement stack, sleep continuity often returns close to pre-perimenopause baseline. For women who use lifestyle alone, improvement is real but partial.
You will not sleep the way you slept at thirty. You can sleep well enough that the day belongs to you again.
The reframe worth carrying with you
For years, perimenopause insomnia was told to women as a moral failing. You should relax more. You should worry less. You should be grateful. The problem is that none of these interventions target the mechanism, and none of them acknowledge that a specific, measurable, hormone-driven change is happening in the sleep architecture of a woman in her forties.
Naming the mechanism changes the experience. You are not broken. You are transitioning through a well-documented, neurobiologically specific window during which the hormone that used to guarantee your sleep is no longer available in the same quantity. This is not permanent. It is not who you are. It is a stage.
The 3am hour will lose its weight. Not by force, but by understanding what it is.
GetClariSync Sleep Desk
Editorial Research · Sleep Science
The GetClariSync Sleep Desk reviews peer-reviewed research in sleep science, chronobiology, and circadian medicine. We focus on journals indexed in PubMed — including Sleep, Sleep Medicine Reviews, Nature Communications, the Journal of Sleep Research, and the Journal of Clinical Sleep Medicine. Each article cites its primary sources, distinguishes correlational findings from causal evidence, and is reviewed for accuracy before publication. We update articles when stronger evidence emerges and post a correction note when we change a substantive claim. We are editorial researchers, not clinicians — for medical concerns, sleep disorders, or persistent insomnia please consult a board-certified sleep physician or your primary care provider.





