On May 12, 2026, a paper in The Lancet quietly corrected one of medicine's longest-running naming errors. 91 years. 170 million women. One organ blamed for a problem it didn't cause.
PCOS (polycystic ovary syndrome) was officially renamed PMOS (polyendocrine metabolic ovarian syndrome) in The Lancet on May 12, 2026. The change reflects a fundamental shift in understanding: the condition was never primarily about ovarian cysts. It is driven by multiple interacting hormonal systems: insulin resistance, androgen excess, and neuroendocrine dysregulation, with effects on metabolism, skin, reproduction, and mental health. Up to 70% of people with PMOS remain undiagnosed. The new name is the first step toward fixing that.
On the morning of May 12, 2026, a paper landed in The Lancet that made 91 years of confusion suddenly make sense. For nearly a century, a condition affecting 1 in 10 women worldwide had been named after the wrong thing. Doctors looked at ovaries enlarged and full of small follicles and called them polycystic. The name stuck. It shaped how the condition was taught, diagnosed, and treated across generations of medical training. The real problem, hidden in insulin pathways, androgen feedback loops, and the complex hormonal circuits connecting them, was present in nearly every blood test. But the name kept pointing clinicians toward an organ that was, in most cases, simply responding to a storm it didn't start.
The Cysts That Were Never Cysts
In 1935, two American gynaecologists named Irving Stein and Michael Leventhal published a paper titled 'Amenorrhea Associated with Polycystic Ovaries.' They had observed seven women with absent periods, excess body hair, and obesity. On examination, their ovaries were enlarged and visually striking — dotted with small round structures that, under the technology of the 1930s, looked like cysts. The name polycystic ovary syndrome followed. It was logical given what they could see. It was also wrong about what those structures actually were.
What Stein and Leventhal called cysts were not pathological formations. They were ovarian follicles — tiny sacs that normally develop around an egg before ovulation — that had simply stopped growing at an immature stage. They were not dangerous structures that could burst. They did not require surgical treatment. They were not unique to the condition. They were the symptom of ovulation that never happened, caused by a hormonal environment that made it impossible for follicles to reach maturity. The ovary was showing a downstream effect. The name immortalized the downstream effect and ignored everything upstream.
A 'polycystic' ovary on ultrasound shows 12 or more antral follicles (small, immature egg-containing sacs) measuring 2–9mm in diameter, or an ovarian volume greater than 10cm³. These follicles are not pathological cysts — they do not rupture, do not cause internal bleeding, and are not a structural defect of the ovary. They represent follicles that arrested development due to the hormonal environment preventing ovulation. Notably, this appearance is also seen in 20–30% of women without PMOS, and some women with PMOS do not show this pattern on ultrasound at all.
“The term PCOS is inaccurate, implying pathological ovarian cysts, obscuring diverse endocrine and metabolic features, and contributing to delayed diagnosis, fragmented care, and stigma, while curtailing research and policy framing.”
What PMOS Actually Stands For — And Why Every Letter Finally Matters
The new name, Polyendocrine Metabolic Ovarian Syndrome, was not chosen because it sounds better. Every word in it was selected to accurately describe what the condition actually involves. Breaking it apart reveals something important: this is a condition that affects multiple hormonal systems, carries significant metabolic risk, and involves the ovaries as one of several affected organs, not the origin of the problem.
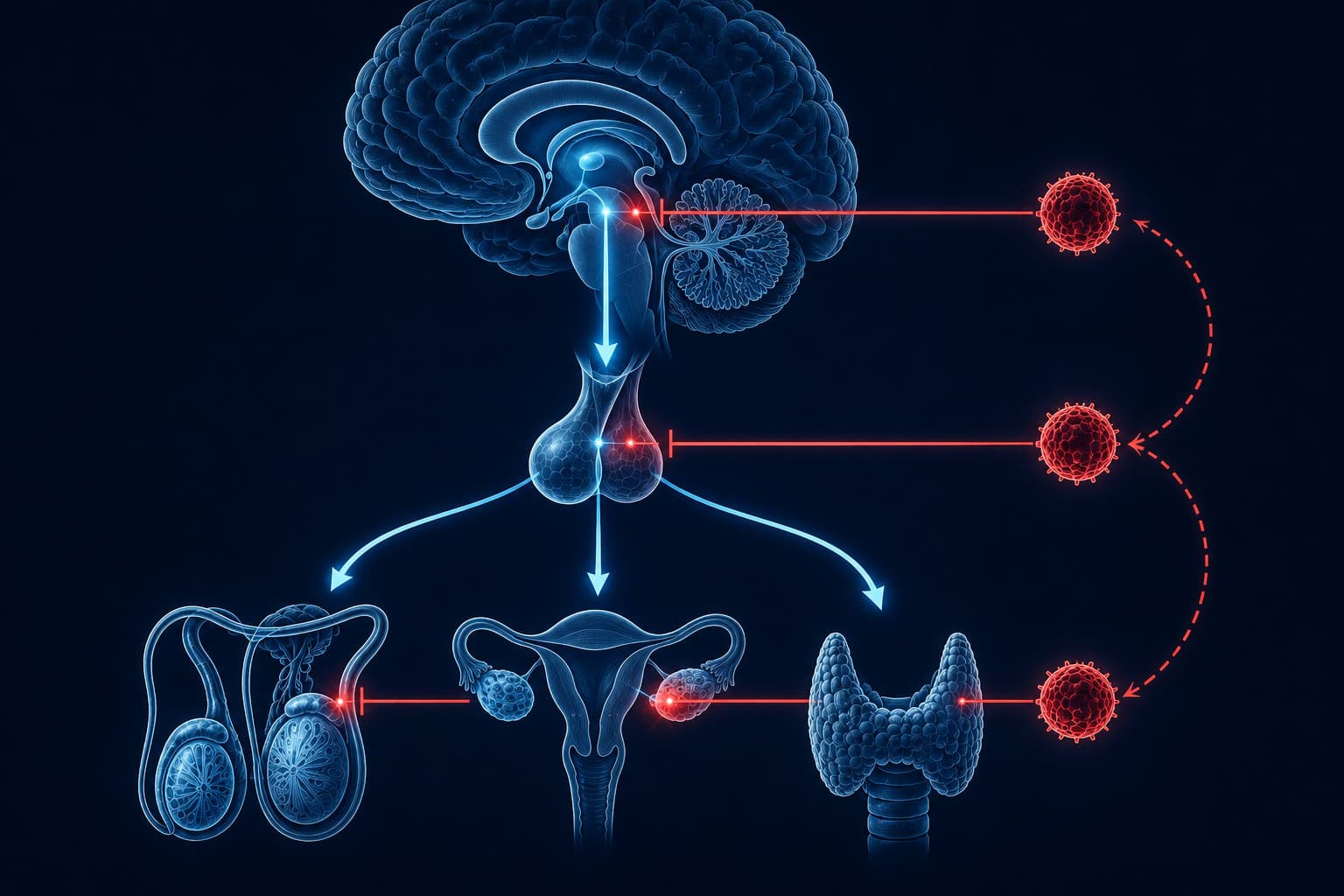
POLY-ENDOCRINE: The condition involves multiple interacting endocrine (hormonal) axes simultaneously: insulin signalling, androgen (testosterone) production, LH/FSH (luteinising and follicle-stimulating hormones) imbalance, and neuroendocrine dysregulation. It is not a single-hormone problem. METABOLIC: An estimated 85% of people with PMOS have insulin resistance. The metabolic consequences include significantly elevated risk of type 2 diabetes, non-alcoholic fatty liver disease, and cardiovascular disease. OVARIAN: The ovaries are involved (ovulatory dysfunction and follicular arrest are defining features), but they are not the origin of the dysfunction. SYNDROME: A constellation of signs and symptoms that can present differently in different people. No two PMOS presentations are identical.
The Vicious Cycle Nobody Drew on the Whiteboard
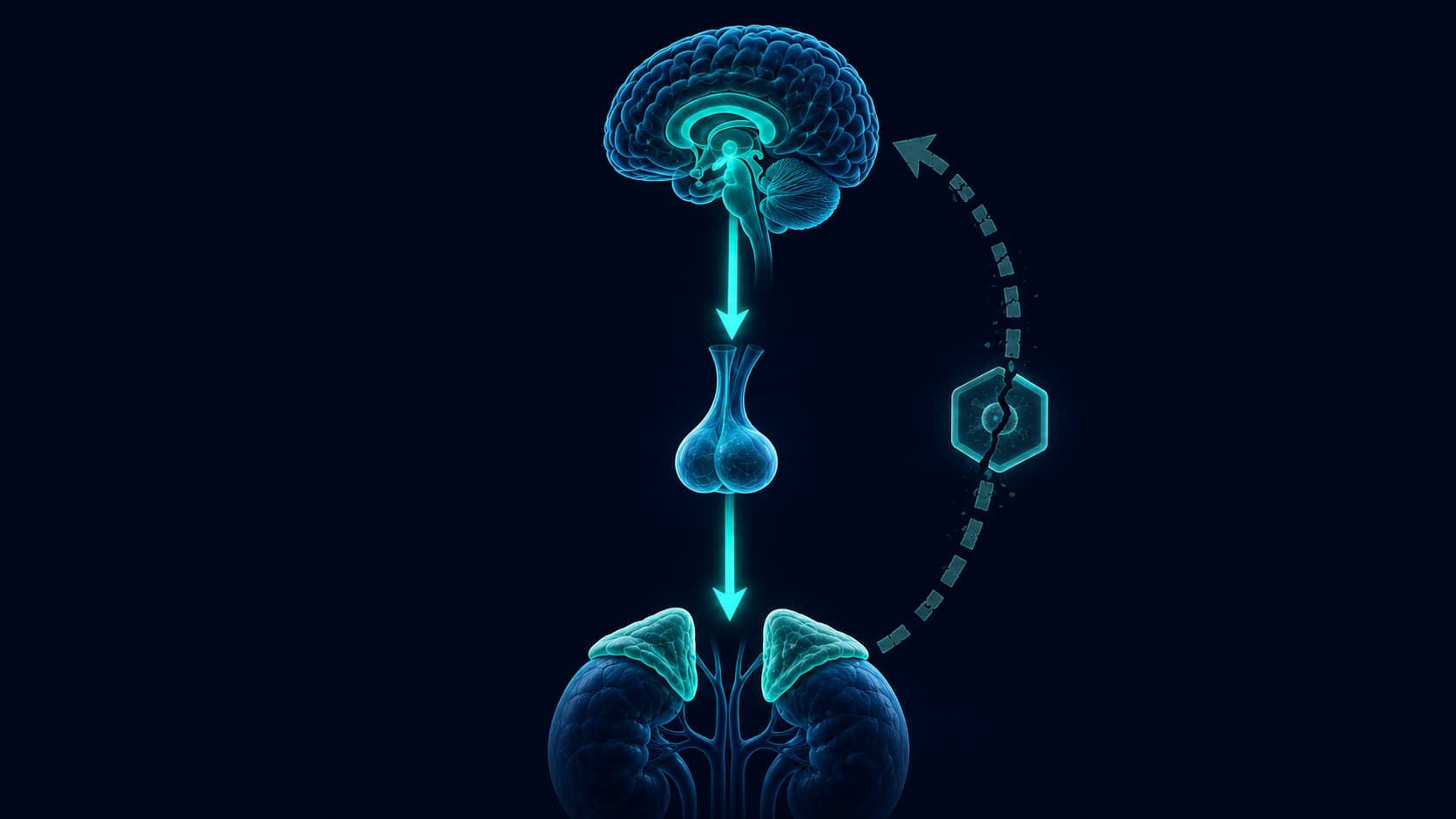
Here is the mechanism that the old name obscured for decades. In PMOS, insulin resistance means the body produces more insulin than usual to achieve the same glucose-lowering effect. That excess insulin travels to the ovaries. Ovarian theca cells (the cells that produce androgens, including testosterone) have insulin receptors. High insulin activates these cells directly, causing them to produce more testosterone. Excess testosterone suppresses a liver protein called sex hormone-binding globulin (SHBG), which normally keeps testosterone inactive in the blood. Less SHBG means more free testosterone circulating. More free testosterone disrupts ovulation, causes acne, drives hair growth in unwanted places, and thins the hair on the scalp. And higher testosterone levels make insulin resistance worse, which produces more insulin, which makes the ovaries produce more testosterone. The loop closes on itself.
Research published in Scientific Reports confirmed the vicious cycle model: insulin and LH act together on ovarian theca cells to enhance androgen biosynthesis. Insulin simultaneously suppresses hepatic SHBG production, increasing free testosterone. Elevated androgens then worsen insulin resistance at the tissue level, sustaining elevated insulin, which restarts the cycle. This explains why symptoms can escalate over time without intervention, and why treating insulin resistance (through lifestyle or medication) often reduces androgen-related symptoms even before addressing the ovaries directly.

Why 70 Percent of People with PMOS Still Don't Know They Have It
The name PCOS sent a clear signal to both patients and clinicians: this is a gynaecological problem. If a woman had irregular periods, she saw a gynaecologist. If she had acne, she saw a dermatologist. If she had weight that wouldn't move despite effort, she was often told to try harder. If she had depression or anxiety (which occur at roughly twice the rate in PMOS), she saw a mental health professional. Each specialist treated their piece of the picture. Nobody was looking at the full system. The name made sure of that.
- Irregular or absent periods dismissed as 'stress' without hormonal investigation
- Acne in adult women treated as a skincare problem, not an endocrine signal
- Hair thinning on scalp treated cosmetically while androgen levels went untested
- Difficulty losing weight attributed to behaviour rather than insulin resistance
- Anxiety and depression treated without investigation of the hormonal driver
- Infertility investigated without looking at the full metabolic picture
- Excess facial or body hair treated aesthetically while underlying hyperandrogenism went unaddressed
The Lancet consensus paper noted that the fragmented care produced by the wrong name was not a failure of individual clinicians. It was a structural failure built into the diagnosis itself. A condition named after ovarian cysts will always be routed primarily through reproductive medicine. A condition named for its actual mechanism (polyendocrine, metabolic, ovarian) creates a different clinical pathway. The rename is, in this sense, a clinical infrastructure change disguised as a linguistic one.
The Skin Signals That Were Hormonal All Along
One of the most practically significant aspects of PMOS is what it does to skin, and how systematically those skin signals were misread. The insulin-androgen vicious cycle described above has a direct dermatological expression. Elevated free testosterone increases sebum (oil) production in the skin's sebaceous glands, promotes follicular hyperkeratinisation (the clogging of pores with excess skin cells), and drives inflammatory acne, particularly along the jawline, chin, and neck. This is not hormonal acne in the colloquial sense. It is a measurable, mechanistic consequence of androgen excess. A 2025 systematic review and meta-analysis found that 43% of women with PMOS have acne, compared to 21% in the general female population.
When Skin Is the First Signal
Persistent adult acne concentrated on the lower face and jaw, especially when accompanied by any of the following, may be worth investigating hormonally: irregular periods, difficulty with weight management, excess facial or body hair, hair thinning at the crown or temples. A dermatologist treating PMOS-related acne will generally look at free testosterone, SHBG, fasting insulin, and LH/FSH ratio, not just topical options. Hormonal acne that does not respond to conventional skincare is frequently an endocrine issue, not a skincare one.
High impact
Hirsutism (excess hair growth on the face, chest, or abdomen) affects a significant proportion of people with PMOS and is similarly a direct consequence of elevated free androgens, not a cosmetic coincidence. Androgenic alopecia — progressive hair thinning beginning at the part line or temples — follows the same mechanism in reverse: DHT (a potent form of testosterone) shortens the hair growth cycle and miniaturises follicles. Both conditions can often be improved by addressing the underlying hormonal environment, rather than treating the surface symptom alone.
The Three Faces of PMOS: One Condition, Many Presentations
One of the reasons PMOS went undiagnosed so often is that it presents differently in different people. The new PMOS framework formalises three dominant phenotypes, allowing clinicians to tailor investigation and treatment rather than applying a single protocol to a condition that can look completely different from one person to the next.
- 1Metabolic-Dominant PMOS Insulin resistance is the primary driver. Characteristic signs: weight that accumulates centrally despite effort, fasting glucose that trends high, dark skin patches at neck or armpits (acanthosis nigricans), fatigue after carbohydrate-heavy meals. Periods may be irregular but are not always absent. First-line focus: insulin sensitisation through dietary changes, physical activity, and in some cases prescription medication discussed with a physician.
- 2Androgen-Dominant PMOS Excess testosterone expression is the primary visible feature. Characteristic signs: persistent adult acne on the jaw and chin, excess facial or body hair, hair thinning at the scalp crown. Insulin resistance may be present but is not the dominant initial presentation. Free testosterone and SHBG are the key markers. Hormonal and dermatological approaches are typically first-line.
- 3Reproductive-Dominant PMOS Ovulatory dysfunction is the primary presenting feature. Characteristic signs: very irregular or absent periods (oligomenorrhea or amenorrhea), difficulty conceiving, multiple small follicles visible on ovarian ultrasound. Metabolic and androgen markers may be mild or within normal range. Reproductive endocrinology and ovulation induction are typically first-line.

What Actually Changes Now That Medicine Got the Name Right
The name change is not immediate. The Lancet consensus paper outlines a three-year transition period before PMOS replaces PCOS in the International Classification of Diseases in 2028. In the meantime, both names will coexist — which means patients may still receive a 'PCOS' diagnosis from clinicians who haven't yet made the shift. What changes is the framing: a diagnosis of PMOS should trigger investigation of all three axes (endocrine, metabolic, reproductive) rather than routing the patient exclusively through gynaecology. For the 70% currently undiagnosed, that reframing could be the difference between a decade of fragmented care and an accurate diagnosis within the first appointment.
Global consensus paper published. 56 international organisations, 22,000 survey responses, 14 years of process. PMOS officially proposed as the replacement name.
Endocrine societies, gynaecology associations, dermatology boards, and primary care bodies begin updating diagnostic guidelines. Medical education starts incorporating PMOS framework.
Health systems update patient-facing materials, diagnostic codes, and clinical pathways. Research funding redirected to reflect PMOS's multi-system nature.
PCOS officially replaced by PMOS in the International Classification of Diseases — the global standard for medical coding, insurance, research funding, and clinical records.
It took 14 years, 22,000 survey responses from patients, 56 international organisations, and a global Delphi consensus process to change four letters. The most meaningful medical renaming in decades came from patients insisting the name of their condition was wrong, and being right.
For anyone who has spent years being told their acne is a skincare issue, their weight is a willpower issue, or their irregular periods are stress — and has a quiet suspicion that something systemic was being missed — the science of PMOS is not an academic update. It is a clinical framework that finally describes the whole picture. The ovary was always a messenger. The message was always in the metabolism.
What PCOS Said About You
- Your ovaries have abnormal cysts
- This is primarily a reproductive disorder
- See a gynaecologist
- The ovary is the problem
- Symptoms are isolated: treat acne separately, treat periods separately
- Fragmented care across multiple unconnected specialists
What PMOS Actually Says
- Multiple hormonal systems are dysregulated
- This is an endocrine, metabolic, and reproductive condition
- Requires multidisciplinary assessment
- The ovary is responding to upstream hormonal disruption
- Symptoms are connected: insulin drives androgen drives skin drives cycle
- Integrated care addressing the root mechanism

- 1Your diagnosis is still valid PCOS and PMOS describe the same condition. If you were diagnosed with PCOS, you have PMOS. The criteria have not changed, only the name and the clinical framework around it.
- 2Ask about insulin resistance If you have not had a fasting insulin test (not just fasting glucose), ask for one. 85% of people with PMOS have insulin resistance, and it frequently goes untested because it is not standard in PCOS workups.
- 3The skin and hair symptoms have a hormonal answer Adult jawline acne, scalp thinning, and excess facial hair are not cosmetic problems requiring cosmetic solutions. They are androgen-driven symptoms that respond to treatment of the underlying hormonal environment.
- 4Mental health is part of the picture Depression and anxiety occur at approximately twice the rate in PMOS. This is not incidental. Research indicates bidirectional relationships between hormonal dysregulation, insulin signalling, and mood. It deserves investigation alongside the physical symptoms, not separately.
- 5The 70% undiagnosis rate means this applies to people you know If someone in your life has unexplained acne, persistent weight difficulty, irregular cycles, or hair concerns, and has never been investigated hormonally, this article is worth sharing.
The Body Science Brief — Every Week
New research, explained clearly. The science your doctor hasn't had time to read yet — in your inbox every week.
Subscribe freeGetClariSync Body Desk
Editorial Research · Sports & Movement Science
The GetClariSync Body Desk reviews research in exercise physiology, recovery science, and sports nutrition. We follow journals including Medicine & Science in Sports & Exercise, the Journal of Applied Physiology, the British Journal of Sports Medicine, and the European Journal of Applied Physiology. We separate findings from trained-athlete populations from those relevant to recreational readers, and we flag when transferring a protocol across populations is unsupported. We are editorial researchers, not certified trainers, physiotherapists, or sports physicians — please consult a qualified professional before starting new exercise programs, especially with existing injuries, pregnancy, cardiovascular conditions, or chronic disease.